
Key messages
- In 2018–19, an estimated 31% (151,000) of Aboriginal and Torres Strait Islander adults had high blood pressure based on both measured and reported data.
- In 2018–19, Indigenous males were more likely to have high measured blood pressure (25%) than Indigenous females (21%). Indigenous males were also more likely to have high measured blood pressure that they did not report—76% compared with 74% for females.
- The rate of high blood pressure for Indigenous adults based on both measured and reported data was similar in remote areas (32%) and non-remote areas (31%).
- In 2018–19, Indigenous Australians had a higher rate of high blood pressure than non-Indigenous Australians in every age group—the largest difference (14 percentage points) among those in the 45–54 age group.
- Prolonged high blood pressure could cause damage to the heart and other organs, known as hypertensive disease. The rate of hospitalisation due to hypertensive disease for Indigenous Australians was higher in remote than non-remote areas—149 per 100,000 compared with 46 per 100,000 population respectively.
- From 2009–10 to 2018–19, there was a 51% increase in the age-standardised rate of hospitalisation for hypertensive disease for Indigenous Australians. The rate difference in hospitalisation between Indigenous Australians and non-Indigenous Australians increased from 43 to 67 per 100,000 population over the period, resulting in a widening of the gap.
- A review into the effectiveness of programs promoting cardiovascular health for Indigenous Australians identified integration with existing services and culturally appropriate delivery models to be common features of an effective program.
Why is it important?
High blood pressure, also referred to as hypertension, is a major risk factor for stroke, coronary heart disease, heart failure, kidney disease, deteriorating vision and peripheral vascular disease leading to leg ulcers and gangrene. High blood pressure is defined as a systolic blood pressure greater than 140 mmHg and/or diastolic pressure greater than 90 mmHg and/or patient receiving medication for high blood pressure (National Heart Foundation of Australia 2016). Major risk factors for high blood pressure include increasing age, family history, poor diet (particularly a high salt intake), obesity, excessive alcohol consumption, and insufficient physical activity (AIHW 2015a, 2015b, 2019). A number of these risk factors are more prevalent among Aboriginal and Torres Strait Islander people (see measures 2.16 Risky alcohol consumption, 2.18 Physical activity, and 2.19 Dietary behaviour, Tier 2 – Health Behaviours).
Reducing the prevalence of high blood pressure is one of the most important means of reducing serious cardiovascular (circulatory) diseases, which are among the leading causes of death for Indigenous Australians (see measure 1.23 Leading causes of mortality).
Burden of disease
In 2018, high blood pressure was estimated to be responsible for 4.3% (10,382 attributable DALY) of the total disease burden for Indigenous Australians, and this proportion increased with age. Total burden due to high blood pressure was highest among those aged 45–64 years for both Indigenous males and females (AIHW 2022a, 2022b).
Among Indigenous Australians, 84% of total disease burden attributed to high blood pressure was due to premature death (that is, fatal burden). There were 348 deaths attributable to high blood pressure (9.6% of total deaths) for Indigenous Australians, equivalent to 8,729 years of life lost due to premature death.
Among Indigenous Australians, 62% of the burden due to hypertensive heart disease in 2018 was attributed to high blood pressure. High blood pressure also contributed to 41% of the burden of coronary heart disease, 39% of stroke burden, 32% of atrial fibrillation & flutter burden and 30% of chronic kidney disease burden.
In 2018, high blood pressure was one of the leading risk factors contributing to the gap in attributable disease burden, accounting for 6.5% of the health gap between Indigenous and non-Indigenous Australians (AIHW 2022a).
Data findings
Indigenous adults with high blood pressure
In 2018–19, the National Aboriginal and Torres Strait Islander Health Survey collected both measured blood pressure and reported blood pressure. For measured blood pressure, the imputation of values was used to correct for those who did not have measurements collected (ABS 2019). Based on both measured and reported data, 31% (an estimated 151,000) of Indigenous adults were estimated to have high blood pressure (140/90 mmHg or higher).
After adjusting for differences in the age structure of the two populations, Indigenous adults were 1.3 times as likely to have high blood pressure compared with non-Indigenous adults—37% (151,000) compared with 29% (5,589,000) respectively. For measured data only (i.e. not including reported), Indigenous adults were 1.2 times as likely as non-Indigenous adults to have high blood pressure (Table D1.07.1).
Undiagnosed and controlled high blood pressure
In 2018–19, of the 486,300 Indigenous adults who had their blood pressure measured (or imputed values used), 23% (an estimated 112,000 adults) had high blood pressure and another 37% (an estimated 180,000) had blood pressure elevated above normal levels, but not considered high (pre-hypertensive; between 120/80 to 140/90 mmHg). The remaining 40% that were measured (195,000) had blood pressure within normal ranges (Table D1.07.1, Figure 1.07.1).
Figure 1.07.1: Proportion of Indigenous Australians aged 18 years and over who had their blood pressure measured, by blood pressure status and whether reported high blood pressure, 2018–19
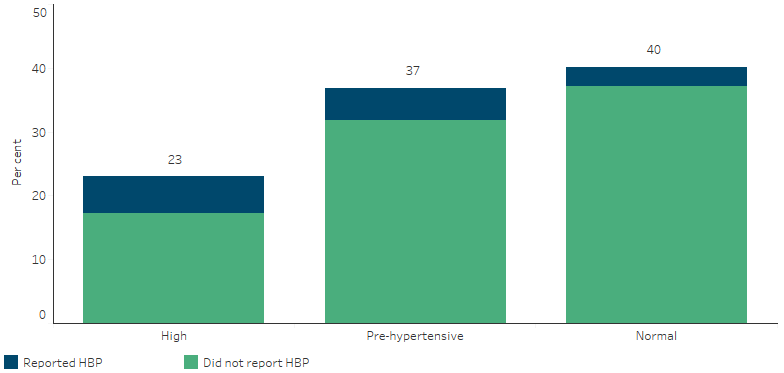
Source: Table D1.07.1. AIHW and ABS analysis of 2018–19 National Aboriginal and Torres Strait Islander Health Survey and National Health Survey 2017–18.
Of the Indigenous adults whose blood pressure was measured as high (112,100), 25% (an estimated 28,000) had reported that they had been diagnosed with high blood pressure. However, 75% (an estimated 84,000) of those with blood pressure measured as high had not reported this to be the case (Table D1.07.2). After adjusting for differences in the age structure of the two populations, the proportion of adults with measured high blood pressure that they had not reported was lower for Indigenous adults than non-Indigenous adults (0.94 times as likely) (Table D1.07.2).
Indigenous Australians who had their blood pressure measured in the last 2 years were slightly more likely to report high blood pressure than all Indigenous Australians. Nearly 9 in 10 Indigenous Australians (88% or 429,484) had their blood pressure checked in the last 2 years (D1.07.2).
In 2018–19, of the Indigenous adults who reported having high blood pressure and had their blood pressure measured, 22% (an estimated 14,705) returned results within normal ranges (Table D1.07.1).
Who has high blood pressure?
For all Australians, the likelihood of high blood pressure increases with age. For Indigenous Australians, rates of reported and measured high blood pressure were similar between non-remote (ranging from 9.8 to 58 per 100 persons) and remote areas (ranging from 7.3 to 61 per 100 persons) across age groups. Rates of reported and measured blood pressure were highest for those aged 55 years and over within both the Indigenous and non-Indigenous populations. The rates were higher for Indigenous Australians across all age groups compared with non-Indigenous Australians. The largest gap between Indigenous and non-Indigenous Australians was for those in the 45–54 age group (14 percentage points) (Table D1.07.7, Figure 1.07.2).
Figure 1.07.2: Measured high blood pressure (140/90 mmHg or higher), by Indigenous status and age group, 2018–19
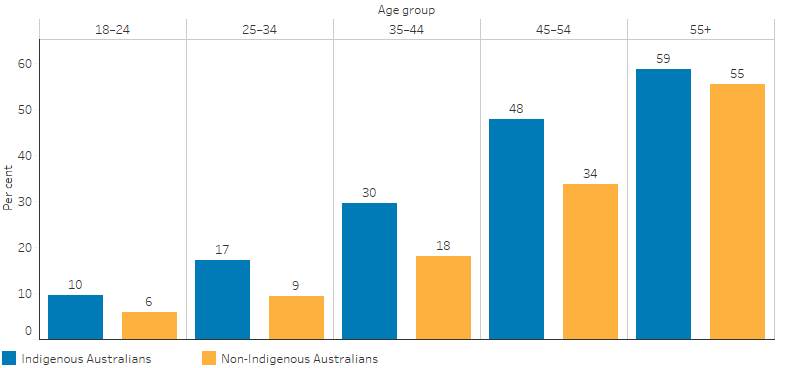
Source: Table D1.07.7. AIHW and ABS analysis of 2018–19 Australian Aboriginal and Torres Strait Islander Health Survey and National Health Survey 2017–18.
The 2018–19 Heath Survey showed that Indigenous males were more likely to have high measured blood pressure (25%) than Indigenous females (21%) (Figure 1.07.3). Indigenous males were also more likely to have high measured blood pressure that they did not report—76% compared with 74% for females (Table D1.07.3).
The rate of high blood pressure for Indigenous adults based on both reported and measured data was similar in remote areas (32%) and non-remote areas (31%) in 2018–19 (Table D1.07.4). Using measured data only also showed the proportion of Indigenous adults with high blood pressure to be similar in remote areas (22%) and non-remote areas (23%) (Table D1.07.3, Figure 1.07.3).
The proportion of Indigenous adults with measured high blood pressure who did not report a diagnosed condition was higher in non-remote areas (75%) compared with remote areas (72%), however this difference was not significant (Table D1.07.3).
Figure 1.07.3: Indigenous Australians aged 18 and over with measured high blood pressure (140/90 mmHg or higher), by sex and remoteness, 2018–19
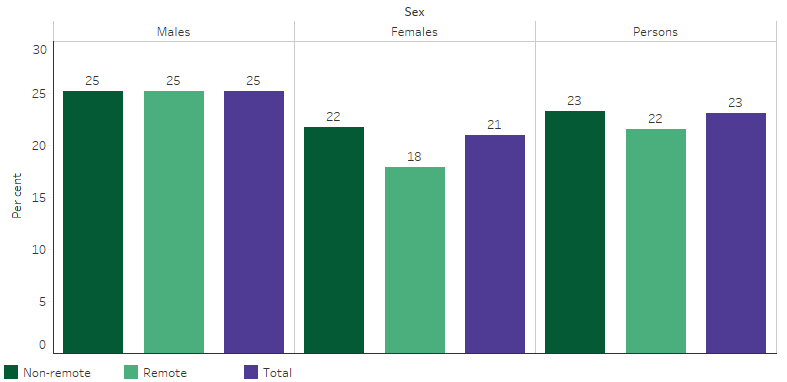
Source: Table D1.07.3. AIHW and ABS analysis of 2018–19 National Aboriginal and Torres Strait Islander Health Survey.
The 2018–19 National Aboriginal and Torres Strait Islander Health Survey showed a number of associations between socioeconomic status and measured and/or reported high blood pressure. Indigenous adults who:
- lived in the most relatively disadvantaged areas were 2.3 times as likely to have high blood pressure (34%) as those living in the most relatively advantaged areas (15%).
- were obese were 1.7 times as likely as those not obese to have high blood pressure (40% compared with 23%).
- considered their health to be fair/poor were 1.9 times as likely as those reporting excellent/very good/good health to have high blood pressure (48% compared with 25%).
- reported having diabetes were 2.3 times as likely to have high blood pressure as those who did not have diabetes (61% compared with 26%).
- reported having kidney disease were twice as likely to report having high blood pressure than those who did not have kidney disease (62% compared with 30%) (Table D1.07.5).
High blood pressure managed by a general practitioner
Most diagnosed cases of high blood pressure are managed by general practitioners (GPs) or medical specialists. According to the Bettering the Evaluation and Care of Health (2010–15) survey, high blood pressure represented 3.6% of problems managed by GPs for Indigenous patients (Table D1.05.5). This compared with 5% for Other Australians. Other Australians are people who have declared they are non‑Indigenous and those whose Indigenous status is unknown. After adjusting for differences in the age structure between the two populations, rates were similar for Indigenous (83 per 1,000 encounters) and Other Australians (85 per 1,000 encounters) (Table D1.07.12).
High blood pressure and management of type 2 diabetes
High blood pressure is common among people with diabetes and it is recommended it be checked regularly. Recommendations are that people with normal blood pressure be checked every six months, those with high blood pressure be checked every three months and people currently changing blood pressure medication be checked every 4 – 8 weeks (Diabetes Australia 2020). In December 2018, Commonwealth-funded Indigenous-specific primary health-care organisations provided national Key Performance Indicators data based on best practice guidelines. In the 6 months to December 2018, of the 43,740 regular clients with type 2 diabetes, 65% (28,447) had their blood pressure assessed. Of those who had their blood pressure assessed, 12,202 (43%) had results in the recommended range (less than or equal to 130/80mmHg) (Table 3.05.16).
Hospitalisation for hypertensive disease
Prolonged high blood pressure could cause damage to the heart and other organs, known as hypertensive disease (AIHW 2022c). Between July 2017 and June 2019, there were 1,079 hospitalisations (0.1% of all hospitalisations) of Indigenous Australians with a principal diagnosis of hypertensive disease and 25,790 for non-Indigenous Australians.
The overall hospitalisation rate for hypertensive disease was 83 hospitalisations per 100,000 population for Indigenous females and 47 hospitalisations per 100,000 population for Indigenous males. Hospitalisation rates for hypertensive disease among Indigenous Australians increased with age. Indigenous females had a higher rate of hospitalisation due to hypertensive disease than Indigenous males for all ages except for young people aged 15–24 years (Table D1.07.9, Figure 1.07.4).
Figure 1.07.4: Hospitalisation rates for hypertensive disease (based on principal diagnosis) for Indigenous Australians, by age group and sex, Australia, July 2017 to June 2019
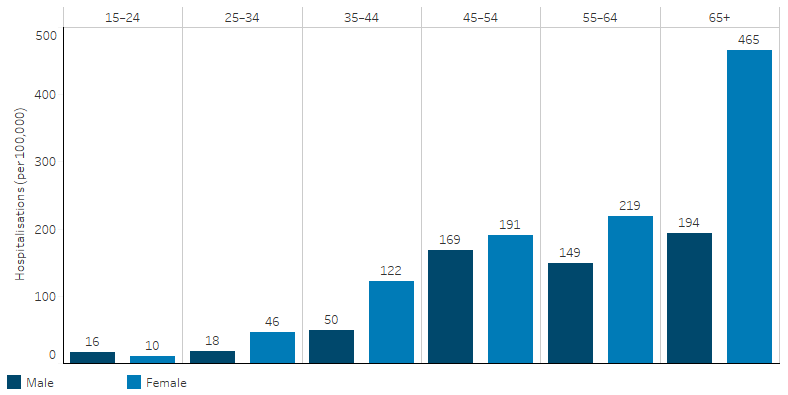
Source: Table D1.07.9. AIHW analysis of National Hospital Morbidity Database.
The rate of hospitalisation for hypertensive disease was higher for Indigenous Australians than non-Indigenous Australians across all age groups. After adjusting for differences in the age structure between the two populations, the rate of hospitalisation due to hypertensive disease for Indigenous Australian was 2.5 times the rate of non‑Indigenous Australians. The greatest difference in hospitalisation rates between the two populations was for those aged 45–54 years, where the rate for Indigenous Australians was 4.7 times the rate for non-Indigenous Australians (Table D1.07.9, Figure 1.07.4).
The rate of hospitalisations due to hypertensive disease for Indigenous Australians was higher in remote than non-remote areas: 149 hospitalisations per 100,000 population compared with 46 per 100,000, respectively (Figure 1.07.5). After adjusting for differences in the age structure between the two populations, Indigenous Australians living in remote areas were hospitalised for hypertensive disease at 4 times the rate of non-Indigenous Australians; in non-remote areas, the rate for Indigenous Australians was 1.9 times as high (Table D1.07.14).
The rate of hospitalisations due to hypertensive disease for Indigenous Australians varied across jurisdictions, from 34 per 100,000 population in Victoria to 135 per 100,000 population in the Northern Territory (Table 1.07.14). The greatest difference in hospitalisation rate was in Western Australia, with the rate for Indigenous Australians 5 times the rate for non-Indigenous Australians (Table D1.07.10).
Figure 1.07.5: Hospitalisation rates for hypertensive disease (based on principal diagnosis) for Indigenous Australians, by jurisdiction and remoteness, Australia, July 2017 to June 2019
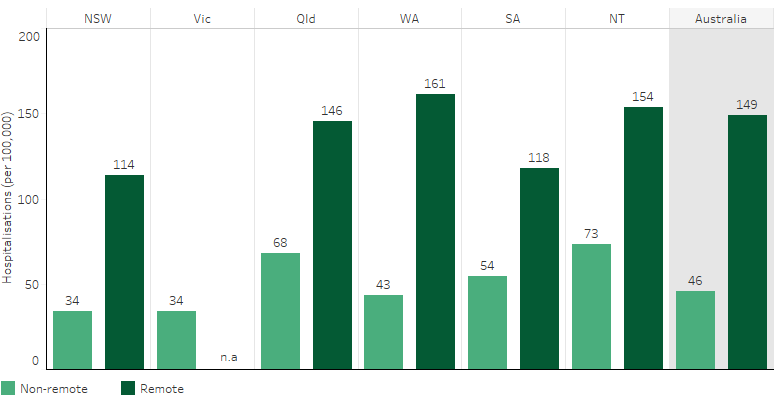
Note: Due to small numbers, Remote areas of Victoria are excluded from the remote category and instead included in the non-remote category. Data for the Australian Capital Territory and Tasmania are not published for confidentiality and/or reliability reasons, but are including in the ‘Australia’ totals.
Source: Table D1.07.14. AIHW analysis of National Hospital Morbidity Database.
Change over time
Looking at burden of disease statistics, between 2003 and 2018, there was a 45% reduction in age-standardised total burden attributable to high blood pressure (from 41 to 23 per 1,000 population). The age-standardised rate of disease burden attributed to high blood pressure declined for both Indigenous and non-Indigenous Australians, with Indigenous Australians having 2.8 times the rate of non-Indigenous Australians in 2018 (as compared with 2.6 times in 2003) (AIHW 2022a).
Looking at hospitalisations data, over the decade from 2009–10 to 2018–19, the (crude) rate of hospitalisation due to hypertensive disease among Indigenous Australians increased from 39 to 68 per 100,000 population. Based on linear regression (which considers all data points in the time period), there was a 64% increase in the hospitalisation rate due to hypertensive disease over the decade. These data are for the 6 jurisdictions with Indigenous identification data of adequate quality (New South Wales, Victoria, Queensland, Western Australia, South Australia, and the Northern Territory).
There was a larger increase in the hospitalisation rate due to hypertensive disease among Indigenous females than Indigenous males over the decade to 2018–19 (92% compared with 30% for males) (Table D1.07.13). In the two-year period from July 2017 to June 2019, the rate for Indigenous females was 1.8 times the rate for Indigenous males (83 compared with 47 per 100,000 population) (Table D1.07.9).
Changes in the rate over time can be affected by ageing of the population. Over the decade 2009–10 to 2018–19, based on age-standardised rates (which adjusts for changes in age-structure over time), the rate of hospitalisations due to hypertensive disease increased by 51% for Indigenous Australians (71% for females, 21% for males), while the rate for non-Indigenous Australians increased by 45% (50% for females, 42% for males). The rate difference in hospitalisation between Indigenous Australians and non-Indigenous Australians increased from 43 to 67 per 100,000 population over the period, resulting in a widening of the gap (Table D1.07.13, Figure 1.07.6).
Figure 1.07.6: Age-standardised hospitalisation rates for a principal diagnosis of hypertensive disease, by Indigenous status, NSW, Vic, Qld, WA, SA and NT, 2006–07 to 2018–19
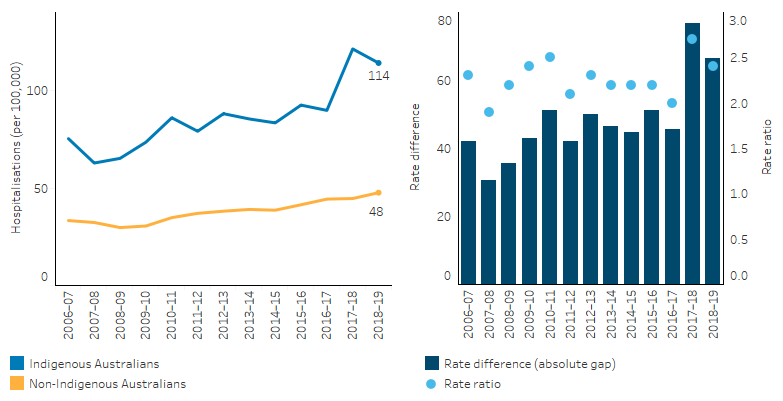
Note: Rate difference is the age-standardised rate (per 100,000) for Indigenous Australians minus the age-standardised rate (per 100,000) for non-Indigenous Australians. Rate ratio is the age-standardised rate for Indigenous Australians divided by the age-standardised rate for non-Indigenous Australians.
Source: Table D1.07.13. AIHW analysis of National Hospital Morbidity Database.
Research and evaluation findings
The findings in this measure showed that high blood pressure is more severe, occurs earlier, and is not controlled as well for Indigenous Australians. Consequently, diseases requiring acute care in hospitals are more common (Table D1.07.9).
A study of Indigenous Australians living in urban Western Australia found that, after controlling for other cardiovascular risk factors, those with high blood pressure were twice as likely to die or be hospitalised due to a cardiovascular event (Bradshaw et al. 2009).
A study in selected remote communities found that the rate of high blood pressure was 3–8 times as high as that in the general population (Hoy et al. 2007). A long-term follow-up study in rural and remote communities in Northern Australia found that the incidence of hypertension in Indigenous adults was nearly double the rate for non-Indigenous adults. Increased incidence of obesity, diabetes and albuminuria (a sign of kidney disease) were found to contribute to this higher rate (Li & McDermott 2015).
High blood pressure is more common among Indigenous Australians than non-Indigenous Australians, and is one of the reasons heart attacks, strokes and other cardiovascular (circulatory) diseases are more common, and cause many more early deaths. While for some people, the propensity to develop high blood pressure appears to be inherited, studies have shown that it can often be prevented or controlled by leading an active and healthy life, remaining fit, preventing obesity, albuminuria and diabetes and, if necessary, taking regular medication (Bunker 2014; Li & McDermott 2015; National Heart Foundation of Australia 2016; Semlitsch et al. 2013).
Studies showed that for those with high blood pressure, treatment with long-term medication can reduce the risk of developing complications, although not necessarily to the levels of unaffected people (AIHW 2015b).
One study in New South Wales found that blood pressure is frequently elevated in urban Indigenous children, aged 2–17 years. The study found that the strongest predictors of blood pressure were parent’s blood pressure and the child’s Body Mass Index. The study recommended family-based interventions to reduce blood pressure in this high-risk group (Larkins et al. 2017).
The use of mobile health digital platforms have the potential to assist in the prevention, treatment and management of a range of health conditions. A mobile health scoping project for screening, managing and preventing cardiovascular disease in Indigenous communities was recently investigated by CSIRO, in partnership with the Queensland Aboriginal and Islander Health Council (QAIHC). The feasibility of a digital platform and app to help provide access to cardiovascular healthcare for Indigenous Australians was explored as a part of the project. The platform has features to monitor blood pressure and manage medication and has capabilities to extend the support of preventive health measures related to physical activity, diet and smoking. Trials sites in regional and remote Aboriginal and Torres Strait Islander Community Controlled Health Organisations were established for a trial to commence in early 2021 (CSIRO 2021).
A study of a cohort of Indigenous Australian women in North Queensland examined pre‑pregnancy factors that predicted hypertension in pregnancy. The study found that pre‑pregnancy obesity and features of the metabolic syndrome (waist circumference of 80cm or more, plus two or more of the following: high triglycerides, high blood pressure, high blood sugar, and low high-density lipoprotein [HDL] cholesterol levels) tracked strongly to increased risk of hypertension, with associated risks to the health of the babies (Campbell et al. 2013).
There is limited evidence on the effectiveness of Indigenous specific high blood pressure prevention and treatment programs particularly in terms of the lasting effects on health outcomes.
In 2018, a review was undertaken into the effectiveness of programs to promote the cardiovascular health of Indigenous Australians. The review found very few cardiovascular health care programs designed specifically for Indigenous Australians. Of those that were identified and found effective, common features of effectiveness included the integration of programs within existing services, provision of culturally appropriate delivery models with a central role for Indigenous Australian Health Workers, and provision of support for communities such as transportation. The review demonstrated that interventions targeted at Indigenous cardiovascular health and related risk factors, such as high blood pressure, can be effective. The results indicated that there are opportunities to improve the cardiovascular health, including a decrease in high blood pressure, of Indigenous Australians at all stages of the disease continuum (Mbuzi et al. 2018). (See measure 1.05 Cardiovascular disease for more information.)
Implications
The survey data reveals that both Indigenous and non-Indigenous Australian populations have large cohorts of adults with undiagnosed high blood pressure. The prevalence of measured high blood pressure among Indigenous adults was estimated at 1.2 times as high as for non-Indigenous adults. The hospitalisation rate was over twice as high, but high blood pressure accounted for a similar proportion of GP consultations for both populations. This suggests that despite higher prevalence, there is an unmet need for primary health care for Indigenous Australians, where high blood pressure can be diagnosed and managed. This could potentially prevent hospitalisations with more advanced illness.
Indigenous Australians aged 45–54 years had the largest gap with non-Indigenous Australians the same age in prevalence of high blood pressure and in hospitalisations for hypertensive disease. Further research is needed into the diagnosis and management of high blood pressure among middle-aged Indigenous Australians and into ways care can be improved for this group. There is a need for earlier, targeted assessment, education and advice about cardiovascular risk factors for Indigenous Australians at a much younger age (such as adolescence) (Mbuzi et al. 2018).
Appropriate diagnosis and management of high blood pressure for Indigenous Australians require access to primary health care with appropriate systems for the identification of Indigenous clients to facilitate the use of Indigenous specific Medicare items for health assessments and chronic disease management. Research into the effectiveness of continuous quality improvement programs in Indigenous primary health care services has demonstrated that blood pressure control and hence cardiovascular disease prevention can be improved by a well-coordinated and systematic approach to chronic disease management (Burgess et al. 2015; McDermott et al. 2003). High blood pressure is often a comorbidity in clients with diabetes and kidney disease, and this comorbidity is a particular focus of the national Key Performance Indicators for Indigenous primary health care.
There is also a need for further research into evidence-based interventions for hypertension that are sensitive to Indigenous Australian culture and needs. Further rigorous evaluation would enable a better understanding of the effectiveness and sustainability of cardiovascular programs among Indigenous Australians (Mbuzi et al. 2018).The National Aboriginal and Torres Strait Islander Health Plan 2021-2031 (the Health Plan), released in December 2021, recognises early access to responsive primary care is also key to addressing the higher hospitalisation rates of Indigenous Australians, where presentation often occurs at a later stage of disease and can lead to higher rates of death. The Health Plan emphasises that action to address cardiovascular disease, diabetes, ear, eye and renal health, and rheumatic heart disease, remain key priorities.
References
-
ABS (Australian Bureau of Statistics) 2019. National Aboriginal and Torres Strait Islander Health Survey, 2018–19. 4715.0. Canberra: ABS.
-
AIHW (Australian Institute of Health and Welfare) 2015a. Cardiovascular disease, diabetes and chronic kidney disease—Australian facts: Aboriginal and Torres Strait Islander people. Canberra: AIHW.
-
AIHW 2015b. Cardiovascular disease, diabetes and chronic kidney disease—Australian facts: risk factors. Canberra: AIHW.
-
AIHW 2019. High blood pressure. Canberra: AIHW.
-
AIHW 2022a. Australian Burden of Disease Study: Impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2018. Canberra: AIHW.
-
AIHW 2022b. Australian Burden of Disease Study 2018: Interactive data on risk factor burden among Aboriginal and Torres Strait Islander people. AIHW. Viewed May 2022.
-
AIHW 2022c. Heart, stroke & vascular diseases. AIHW. Viewed August 2022.
-
Bradshaw PJ, Alfonso HS, Finn J, Owen J & Thompson PL 2009. Coronary heart disease events in Aboriginal Australians: incidence in an urban population. The Medical Journal of Australia 190:583-6.
-
Bunker J 2014. Hypertension: diagnosis, assessment and management. Nursing Standard 28:50-9.
-
Burgess CP, Sinclair G, Ramjan M, Coffey PJ, Connors CM & Katekar LV 2015. Strengthening cardiovascular disease prevention in remote indigenous communities in Australia's Northern Territory. Heart,, Lung & Circulation 24:450-7.
-
Campbell SK, Lynch J, Esterman A & McDermott R 2013. Pre-pregnancy predictors of hypertension in pregnancy among Aboriginal and Torres Strait Islander women in north Queensland, Australia; a prospective cohort study. BMC Public Health 13:138.
-
CSIRO 2021. Mobile health to mitigate Indigenous CVD. Viewed 28/8/2022.
-
Diabetes Australia 2020. Blood pressure. Viewed 09/09/2020.
-
Hoy WE, Kondalsamy-Chennakesavan S, Wang Z, Briganti E, Shaw J, Polkinghorne K et al. 2007. Quantifying the excess risk for proteinuria, hypertension and diabetes in Australian Aborigines: comparison of profiles in three remote communities in the Northern Territory with those in the AusDiab study. Australian & New Zealand Journal of Public Health 31:177-83.
-
Larkins N, Teixeira-Pinto A, Banks E, Gunasekera H, Cass A, Kearnes J et al. 2017. Blood pressure among Australian Aboriginal children. Journal of Hypertension 35:1801-7.
-
Li M & McDermott R 2015. Obesity, albuminuria, and gamma-glutamyl transferase predict incidence of hypertension in indigenous Australians in rural and remote communities in northern Australia. Journal of Hypertension 33:704-9; discussion 9-10.
-
Mbuzi V, Fulbrook P & Jessup M 2018. Effectiveness of programs to promote cardiovascular health of Indigenous Australians: a systematic review. International Journal for Equity in Health 17:153.
-
McDermott R, Tulip F, Schmidt B & Sinha A 2003. Sustaining better diabetes care in remote Indigenous Australian communities. British Medical Journal 327:428.
-
National Heart Foundation of Australia 2016. Guideline for the diagnosis and management of hypertension in adults - 2016. Melbourne: NHFA.
-
Semlitsch T, Jeitler K, Hemkens LG, Horvath K, Nagele E, Schuermann C et al. 2013. Increasing Physical Activity for the Treatment of Hypertension: A Systematic Review and Meta-Analysis. Sports Medicine 43:1009-23.