
Key facts
Why is it important?
The health effects of smoking is evident in the high rates of hospitalisation and deaths from tobacco-related conditions (e.g. chronic lung disease, cardiovascular disease and many forms of cancer) (Marley et al. 2014; Pircher et al. 2012).
In Australia, up to two-thirds of deaths in current smokers can be attributed to smoking, and current smokers are estimated to die an average of 10 years earlier than non-smokers. It has been estimated that around 18,800 Australians die prematurely from tobacco-related diseases each year (AIHW 2016a) and that smoking imposes an estimated $31.5 billion financial burden on the community (Collins & Lapsley 2008).
Smoking cessation reduces mortality, with earlier cessation resulting in greater reductions (Banks et al. 2015).
In 2008, the Council of Australian Governments committed to Closing the Gap in life expectancy between Aboriginal and Torres Strait Islander people and non-Indigenous Australians within a generation (PM&C 2019). With the high rates of smoking among Indigenous Australians, reducing the smoking rates is key to making progress in closing the gap, and has been the focus of significant effort by governments and services.
Burden of disease
Smoking was the leading modifiable risk factor contributing to the burden of disease among Indigenous Australians in 2011, accounting for 12% of the total burden. Around two-fifths of the cancer burden (39%), and the cardiovascular disease burden (39%) and the respiratory disease burden (42%) were attributed to smoking.
Smoking was also the risk factor most responsible for the gap in disease burden between Indigenous and non‑Indigenous Australians in 2011, accounting for 23% of the total gap (AIHW 2016b).
Data findings
Smoking rates
The 2018–19 National Aboriginal and Torres Strait Islander Health Survey (Health Survey) provides the latest data on the rates of smoking among Indigenous Australians. For Indigenous Australians aged 15 and over, just over 4 in 10 Indigenous Australians (41%; 217,200) reported being a current smoker, 37% (200,400) smoked daily and 3% (16,700) smoked less than daily (Table D2.15.4).
Indigenous Australians aged 15 and over were 2.9 times as likely to be a current smoker as non‑Indigenous Australians, after adjusting for differences in the age structure between the two populations (41% compared with 14%) (Table D2.15.7).
Between 2002 and 2018–19, after adjusting for differences in the age structure between the two populations, the smoking rates for Indigenous Australians aged 15 and over declined from 48% to 41%. The smoking rates for non-Indigenous Australians also declined over the period (from 24% to 14%) and there has been no improvement in the gap between the two populations (from 24 percentage points in 2002 to 27 percentage points in 2018–19) (Table D2.15.3, Figure 2.15.1).
Figure 2.15.1: Age-standardised smoking rates, persons aged 15 and over, by Indigenous status, 2002 to 2018–19
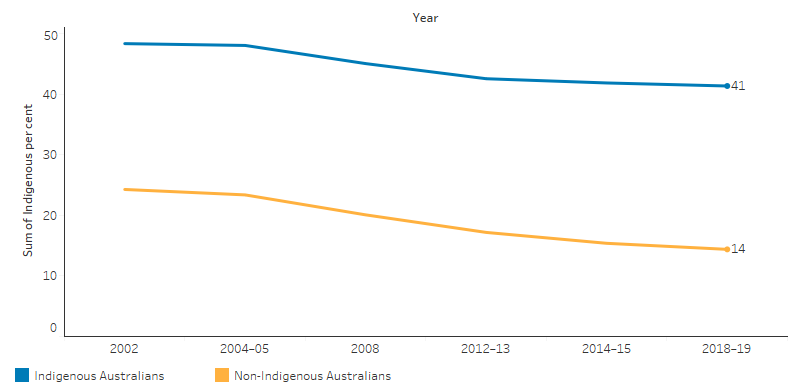
Source: Table D2.15.3. AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Social Survey 2002, 2008, 2014–15; National Health Survey 2001, 2004–05, 2007–08, 2011–12, 2014–15, 2017–18; Australian Aboriginal and Torres Strait Islander Health Survey 2012–13; and National Aboriginal and Torres Strait Islander Health Survey 2004–05, 2018–19.
In 2018–19, the smoking rates for Indigenous Australians was lowest in the 15–17 age group (13%) and highest for those aged 35–44 (50%) (Table D2.15.1, Figure 2.15.2).
Figure 2.15.2: Proportion of Indigenous Australians aged 15 and over reporting they are a current smoker, by age group, 2018–19
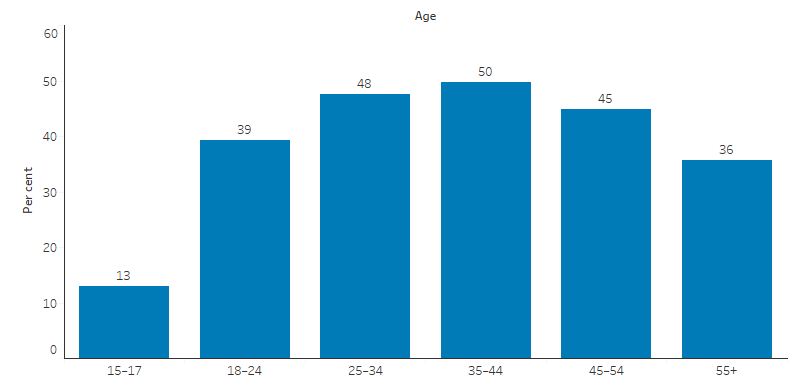
Source: Table D2.15.1. AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Health Survey 2018–19.
The greatest improvements in the smoking rates between 2002 and 2018–19 were seen for younger Indigenous Australians. For Indigenous Australians aged 15–17, the proportions of:
- current smokers fell from 33% to 13% (6,400)
- those who reported never smoking increased from 62% to 85% (41,800) (Table D2.15.4).
In 2018–19, the self-reported smoking rates for Indigenous Australians aged 15 and over was lowest in the Australian Capital Territory (23%) and highest in the Northern Territory (54%) (Table D2.15.7, Figure 2.15.3).
Figure 2.15.3: Age-standardised proportion of Indigenous Australians aged 15 and over who were current smokers, by jurisdiction and Indigenous status, 2018–19
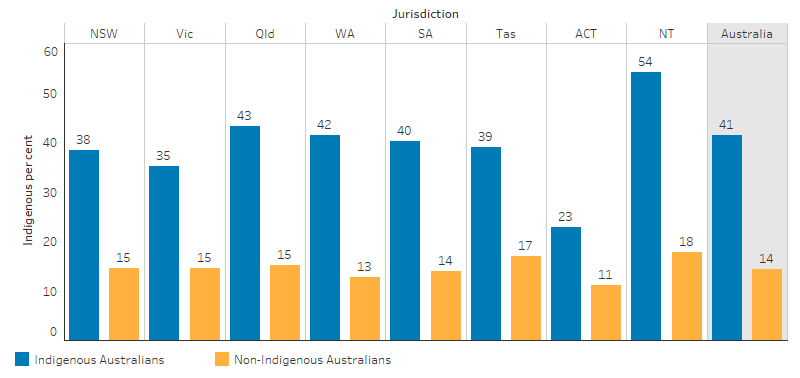
Source: Table D2.15.7. AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Health Survey 2018–19 and National Health Survey 2017–18.
By remoteness, the proportion of Indigenous Australians aged 15 and over who currently smoked was lowest in Major cities (29%) and highest in Very remote areas (58%).
Indigenous males had higher rates of smoking than Indigenous females (43% and 38%, respectively). The difference in the smoking rates for Indigenous males and Indigenous females was greatest in Outer regional areas (55% compared with 41%, respectively) (Table D2.15.1, Figure 2.15.4).
Figure 2.15.4: Proportion of Indigenous Australians aged 15 and over who were current smokers, by remoteness and sex, 2018–19
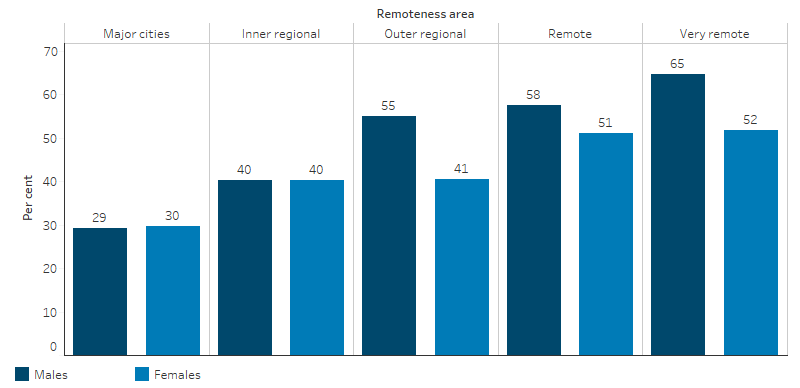
Source: Table D2.15.1. National Aboriginal and Torres Strait Islander Health Survey 2018–19.
Between 2002 and 2018–19, the declines in the smoking rates for Indigenous Australians aged 15 and over were due to changes in Non-remote areas, with a decline of 13 percentage points (from 50% to 37%). However, the smoking rates for Indigenous Australians in Remote areas went up by 1 percentage point between 2002 and 2018–19 (from 55% to 56%) (Table D2.15.4, Figure 2.15.5).
Figure 2.15.5: Age-standardised proportion of Indigenous Australians aged 15 and over who were current smokers, by remoteness, 2002 to 2018–19
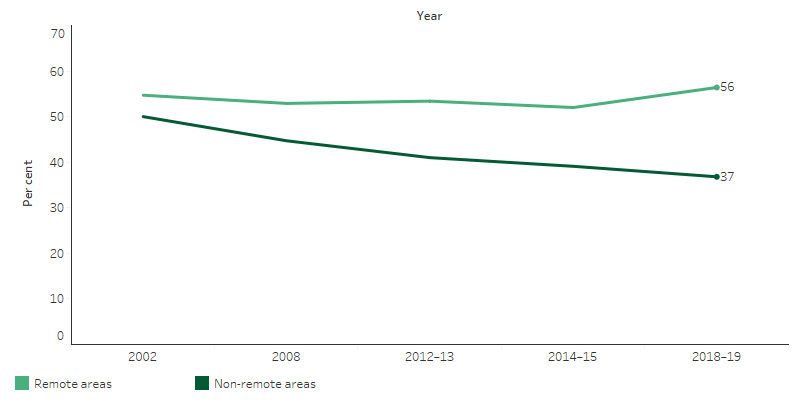
Source: Table D2.15.4. AIHW and ABS analysis of National Aboriginal Torres Strait Islander Social Survey 2002, 2008 and 2014–15, and Australian Aboriginal and Torres Strait Islander Health Survey 2012–13 and National Aboriginal Torres Strait Islander Health Survey 2018–19.
Quitting or reducing smoking
The median number of cigarettes smoked daily by Indigenous smokers declined from 12 in 2008 to 10 in 2018–19 (Table D2.15.2).
In 2018–19, 52% of Indigenous smokers had tried to quit smoking in the previous 12 months (Table D2.15.10). The 2014–15 National Aboriginal and Torres Strait Islander Social Survey explored reasons why Indigenous Australians reduced or quit smoking. The most common reasons for reducing or quitting smoking in the previous 12 months were general health (73%; 92,520), cost (56%; 70,900), to improve fitness (31%; 39,560) and the encouragement of family or friends (27%; 34,060) (Table D2.15.11).
Socioeconomic and health factors associated with smoking
In 2018–19, Indigenous Australians aged 15 and over were more likely to report being a non-smoker if they had completed Year 12 (72%), were employed (67%) or were in the highest (4th or 5th) income quintile (78%) (Table D2.15.16, Figure 2.15.6).
Figure 2.15.6: Proportion of Indigenous Australians aged 15 and over who reported being a non-smoker, by selected socio-economic characteristics, 2018–19
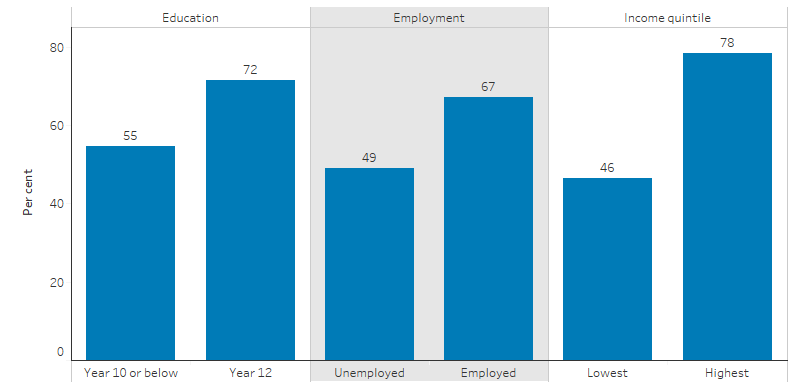
Source: Table D2.15.16. AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Health Survey 2018–19.
In 2018–19, Indigenous Australians aged 15 and over were more likely to report being a smoker if they:
- had high or very high levels of psychological distress (52% compared with 39% for those with low/moderate levels)
- had fair or poor self-assessed health status (48% compared with 32% with excellent/very good (Table D2.15.17).
Indigenous Australians aged 15 and over who smoked were also more likely to drink at risky levels (62% exceeded short-term drinking guidelines compared with 42% for non-smokers) and to use harmful substances (41% compared with 20% of non-smokers) (Table D2.15.18).
In 2014–15, Indigenous Australians aged 15 and over were more likely to report being a smoker if they had experienced one or more stressors in the previous 12 months (45% compared with 35% for those who had not) (Table D2.15.15).
In 2018, 80% (247) of Indigenous prison entrants were current smokers (AIHW 2019) (see measure 2.11 Contact with the criminal justice system).
Indigenous-specific primary health care organisations
The national Key Performance Indicators for Aboriginal and Torres Strait Islander Primary Health Care data collection includes data on the smoking status of 176,033 regular clients aged 15 and over who attend 221 Indigenous-specific primary health care organisations around Australia. In December 2018, 52% (91,374) of regular clients were current smokers. Indigenous regular clients aged 25–34 had the highest proportion of current smokers compared with other age groups (61%; 24,321) (Table D2.15.12, Table D2.15.13).
Research and evaluation findings
Research has shown that smoking increases the risk of coronary heart disease by two to four times, stroke by two to four times, and developing lung cancer by around 25 times (U.S. Department of Health and Human Services 2014). Smoking increases the risk of type 2 diabetes (Pan et al. 2015), a condition relatively common among Indigenous Australians (see measure 1.09 Diabetes). Smoking also leads to adverse oral health outcomes, including chronic gum disease (periodontitis), impaired oral wound healing, and diseases with significant morbidity and mortality, such as oral and oropharyngeal cancer (Do et al. 2008; Zhang et al. 2011).
Maternal smoking during pregnancy increases the risk of poor outcomes for mothers, babies and children (see measures 1.01 Birthweight and 2.21 Healthy behaviours during pregnancy). Pregnancy complications include placenta praevia, abruption placentae, stillbirth, small gestational age infants and preterm births (De Long et al. 2014). A multivariate analysis of 2015–17 perinatal data indicates that, excluding pre-term and multiple births, 47% of low birthweight babies born to Indigenous mothers were attributable to smoking during pregnancy, compared with 12% for non-Indigenous mothers. After adjusting for differences in the age structure of the two populations and other factors, it was estimated that if the smoking rate by Indigenous mothers was the same as that of non-Indigenous mothers, the proportion of low birthweight babies could be reduced by 33% (see measures 1.01 Birthweight and 2.21 Healthy behaviours during pregnancy).
Maternal smoking is linked with low birth weight, an increased risk of sudden infant death syndrome, and renders infants susceptible to more severe respiratory infections (Gunnerbeck et al. 2011; Mohsin et al. 2003; Sawnani et al. 2004). Smoking also promotes the development of allergic diseases by changing the activation profile of immune cells (Gibbs et al. 2016).
The adverse effect of maternal smoking (including mothers exposed to second-hand smoke) can affect their child’s health well into their adolescence and adulthood. Studies have found that adolescents whose mother had smoked or had been exposed to second-hand smoke were more susceptible to obesity, hypertension and type 2 diabetes (de Jonge et al. 2013; Harris et al. 2013; Ino et al. 2012; Jaddoe et al. 2014; Wang et al. 2014). For more information on second‑hand smoke and the adverse health effects for those exposed see measure 2.03 Environmental tobacco smoke.
Research has found that quitting smoking can reduce health risks:
- After one year from quitting smoking, the risk of a heart attack reduces sharply.
- Within two to five years after quitting smoking, the risk of stroke may reduce to about that of a non-smoker.
- Quitting smoking reduces the risks of cancers of the mouth, throat, oesophagus, and bladder by half within five years.
- After 10 years of quitting smoking, the risk of dying from lung cancer drops by half (Office on Smoking and Health (US) 2006).
A 2017 study found the graphic warning labels on cigarette packaging appeared to have a positive effect on Indigenous smokers, who reported that it stopped them from ‘having a smoke’ (Nicholson et al. 2017).
Reasons for smoking appear to be similar for Indigenous men and women while motivations to quit differ (Knott et al. 2016). Predictors for making a quit attempt differ from predictors for sustaining a quit attempt (Nicholson et al. 2017). Predictors of smoking behaviour among adolescents differ for males and females (Mazanov & Byrne 2008).
Nicholson and others (2015) found that Indigenous Australian’s whose local health services had smoking control programs were more likely to have tried to quit, but they were less likely to have sustained quit attempts. Unemployed smokers, those who had not completed year 12 and those from Remote areas were also less likely to sustain a quit attempt (Nicholson et al. 2015).
Studies of smoking cessation in pregnant Indigenous women have found that social and familial influence had a major effect on whether they could give up smoking during pregnancy (Harris et al. 2019).
Other factors that have been identified to help reduce smoking include:
- Implementing a comprehensive program that covers multiple activities (for example pharmacotherapies combined with culturally tailored interventions and health professional support).
- Addressing prevention and cessation at the individual, community and legislative levels (for example brief interventions with community education and smoke-free policies).
- Centring the program on Indigenous leadership; with long-term community investments.
- Providing workforce support and development.
- Implementing culturally appropriate health materials and activities. (Carson et al. 2012; Hearn et al. 2011; Minichiello et al. 2015; Noble et al. 2016; Robertson et al. 2013a)
Tobacco smoking is influenced by a range of social, cultural and family factors, including the normalisation of smoking in peer groups and families, positive attitudes towards smoking, and smoking as a coping mechanism (Hearn et al. 2011; Johnston & Thomas 2008; Robertson et al. 2013b; Scollo & Winstanley 2019). Additional barriers to quitting in remote areas include underlying social disadvantage and access to and uptake of services and treatment to support quitting (Sarin et al. 2015; Thomas et al. 2015). In New South Wales, tobacco outlet density has been found to be higher in more disadvantaged districts and positively correlated with smoking rates (Marashi-Pour et al. 2015).
The effects of colonisation and subsequent government policies have directly led to tobacco use and addiction among Indigenous Australians. For example, colonial processes have contributed to, and continues to contribute to, Indigenous Australians experiencing ongoing trauma and stress, racism and exclusion from economic structures—which are all associated with tobacco smoking (Colonna et al. 2020). Historically, records suggest that colonists exploited Indigenous Australian’s addiction to tobacco, including those who had not previously used native tobacco. Many colonists paid Indigenous Australians tobacco, instead of cash, for their labour (Brady 2002).
The influence of these factors varies across the different community and social settings in which Indigenous Australians live (Johnston & Thomas 2008). Consequently, it is important that tobacco reduction strategies acknowledge the social exchange that occurs while smoking, the important role of family and the high rates of stress experienced by Indigenous Australians (Cosh et al. 2015; Hearn et al. 2011).
The literature on Indigenous populations has found that there is limited rigorous evidence to evaluate which interventions and cessation programs are effective in reducing smoking. No single intervention program or combination of activities will reduce tobacco use in Indigenous communities (Carson et al. 2012; Minichiello et al. 2015).
Colonna and others (2020) suggest that programs could be strengthened through rigorous evaluation evidence, in addition to expanded coverage and long-term funding (Colonna et al. 2020). Sarin and others (2015) stressed that in order for smoking intervention programs to succeed, they should be evidence-based, coordinated, integrated and involve Indigenous Australians and Aboriginal Community Controlled Health Organisations in all aspects of development through to implementation and evaluation (Sarin et al. 2015).
An evaluation of the Tackling Indigenous Smoking (TIS) program found that the program’s flexible design and place-based approach has been effective in reducing the high smoking rates among Indigenous Australians (CIRCA 2019). However, the evaluation highlighted that there was a lack of data and evidence, and there were some challenges in program delivery. Regional grant recipients expressed a desire to have a standardised indicator so they can measure the effect of the program on health outcomes. In terms of program delivery, the competing priorities in the community (particularly in some Remote and rural areas) and a lack of buy-in from senior management, led to delays in the implementation of the TIS.
Implications
Australian governments have worked closely with Indigenous Australians and health organisations over many years to deliver a range of approaches to address the high rates of tobacco smoking in the Indigenous Australian population. The smoking rates are starting to decline; though are still very high, particularly in Remote areas. The lack of progress in Remote areas is cause for concern. Further effort will be needed for sustained reductions in smoking prevalence.
A more local understanding of the smoking prevalence, and barriers to quitting, including among women of reproductive age and those living in Remote areas, will assist in developing and implementing targeted programs. Understanding of the social determinants of health is also important for informing interventions given the association between socioeconomic factors such as education, employment and income and smoking prevalence.
The main indicator used in this measure is the rate of current smoking (daily plus other smokers) among those aged 15 and over. This is because there is no safe level of smoking (Inoue-Choi et al. 2017) and the majority of young Indigenous Australian smokers commenced smoking prior to turning 18 (Heris et al. 2020). Other reports and research sometimes present the data slightly differently, such as to focus on the rates for those aged 18 and over or for daily smokers only. Regardless of these differences, smoking remains very high among Indigenous Australians, and while recent declines are encouraging, sustained effort will be required well into the future to reduce the effect smoking has on the burden of disease for Indigenous Australians.
While some positive health effects of the recent reductions in smoking prevalence may be immediate and within the short term (such as in cardiovascular outcomes), there is a long lag before reductions in smoking prevalence will fully affect smoking-related cancer mortality. This means smoking-related cancer mortality may continue to rise over the next decade before reaching its peak (Lovett et al. 2017).
References
- AIHW (Australian Institute of Health and Welfare) 2016a. Australian Burden of Disease Study: impact and causes of illness and death in Australia 2011. Canberra: AIHW.
- AIHW 2016b. Australian Burden of Disease Study: impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2011. Australian Burden of Disease Study series 6. Cat. no. BOD 7. Canberra: AIHW.
- AIHW 2019. The health of Australia’s prisoners 2018. Cat. no. PHE 246. Canberra: AIHW.
- Banks E, Joshy G, Weber MF, Liu B, Grenfell R, Egger S et al. 2015. Tobacco smoking and all-cause mortality in a large Australian cohort study: findings from a mature epidemic with current low smoking prevalence. BMC medicine 13:38.
- Brady M 2002. Health inequalities: Historical and cultural roots of tobacco use among Aboriginal and Torres Strait Islander people. Australian and New Zealand journal of public health 26:120-4.
- Carson KV, Brinn MP, Peters M, Veale A, Esterman AJ & Smith BJ 2012. Interventions for smoking cessation in Indigenous populations. Cochrane Database of Systematic Reviews 1:CD009046.
- CIRCA (Cultural and Indigenous Research Centre Australia) 2019. Tackling Indigenous Smoking Program Final Evaluation Report, July 2018.
- Collins DJ & Lapsley HM 2008. The costs of tobacco, alcohol and illicit drug abuse to Australian society in 2004/05. (ed., Department of Health and Ageing). Canberra: DoHA.
- Colonna E, Maddox R, Cohen R, Marmor A, Doery K, Thurber K et al. 2020. Review of tobacco use among Aboriginal and Torres Strait Islander peoples.
- Cosh S, Hawkins K, Skaczkowski G, Copley D & Bowden J 2015. Tobacco use among urban Aboriginal Australian young people: a qualitative study of reasons for smoking, barriers to cessation and motivators for smoking cessation. Australian journal of primary health 21:334-41.
- De Jonge LL, Harris HR, Rich-Edwards JW, Willett WC, Forman MR, Jaddoe VWV et al. 2013. Parental Smoking in Pregnancy and the Risks of Adult-Onset Hypertension. Hypertension 61:494-500.
- De Long NE, Barra BG, Hardy DB & Holloway AC 2014. Is it safe to use smoking cessation therapeutics during pregnancy? Expert Opinion on Drug Safety 13:1721-31.
- Do LG, Slade GD, Roberts-Thomson KF & Sanders AE 2008. Smoking attributable periodontal disease in the Australian adult population. Journal of Clinical Periodontology 35:398-404.
- Gibbs K, Collaco JM & McGrath-Morrow SA 2016. Impact of tobacco smoke and nicotine exposure on lung development. Chest 149:552-61.
- Gunnerbeck A, Wikstrom AK, Bonamy AK, Wickstrom R & Cnattingius S 2011. Relationship of maternal snuff use and cigarette smoking with neonatal apnea. Pediatrics 128:503-9.
- Harris BM, Harris ML, Rae K & Chojenta C 2019. Barriers and facilitators to smoking cessation within pregnant Aboriginal and/or Torres Strait Islander women: An integrative review. Midwifery 73:49-61.
- Harris HR, Willett WC & Michels KB 2013. Parental smoking during pregnancy and risk of overweight and obesity in the daughter. International Journal of Obesity 37:1356-63.
- Hearn S, Nancarrow H, Rose M, Massi L, Wise M, Conigrave K et al. 2011. Evaluating NSW SmokeCheck: a culturally specific smoking cessation training program for health professionals working in Aboriginal health. Health Promotion Journal of Australia 22:189-95.
- Heris CL, Eades SJ, Lyons L, Chamberlain C & Thomas DP 2020. Changes in the age young Aboriginal and Torres Strait Islander people start smoking, 2002-2015. Public Health Research & Practice 30.
- Ino T, Shibuya T, Saito K & Inaba Y 2012. Relationship between body mass index of offspring and maternal smoking during pregnancy. International Journal of Obesity 36:554-8.
- Inoue-Choi M, Liao LM, Reyes-Guzman C, Hartge P, Caporaso N & Freedman ND 2017. Association of long-term, low-intensity smoking with all-cause and cause-specific mortality in the National Institutes of Health–AARP Diet and Health Study. JAMA internal medicine 177:87-95.
- Jaddoe VWV, de Jonge LL, van Dam RM, Willett WC, Harris H, Stampfer MJ et al. 2014. Fetal Exposure to Parental Smoking and the Risk of Type 2 Diabetes in Adult Women. Diabetes care 37:2966-73.
- Johnston V & Thomas DP 2008. Smoking behaviours in a remote Australian Indigenous community: The influence of family and other factors. Social Science & Medicine 67:1708-16.
- Knott VE, Gilligan G, Maksimovic L, Shen D & Murphy M 2016. Gender determinants of smoking practice in Indigenous communities: an exploratory study. European Journal of Cancer Care 25:231-41.
- Lovett R, Thurber K & Maddox R 2017. The Aboriginal and Torres Strait Islander smoking epidemic: what stage are we at, and what does it mean? Public Health Research & Practice 27:e2741733.
- Marashi-Pour S, Cretikos M, Lyons C, Rose N, Jalaludin B & Smith J 2015. The association between the density of retail tobacco outlets, individual smoking status, neighbourhood socioeconomic status and school locations in New South Wales, Australia. Spatial and Spatio-temporal Epidemiology 12:1-7.
- Marley JV, Kitaura T, Atkinson D, Metcalf S, Maguire GP & Gray D 2014. Clinical trials in a remote Aboriginal setting: lessons from the BOABS smoking cessation study. BMC Public Health 14:579.
- Mazanov J & Byrne DG 2008. Modelling change in adolescent smoking behaviour: stability of predictors across analytic models. British Journal of Health Psychology 13:361-79.
- Minichiello A, Lefkowitz ARF, Firestone M, Smylie JK & Schwartz R 2015. Effective strategies to reduce commercial tobacco use in Indigenous communities globally: A systematic review. BMC Public Health 16:21.
- Mohsin M, Wong F, Bauman A & Bai J 2003. Maternal and neonatal factors influencing premature birth and low birth weight in Australia. Journal of biosocial science 35:161.
- Nicholson A, Borland R, Bennet PT, Davey MA, Sarin J, Van der Sterren A et al. 2017. The Effect of Pack Warning Labels on Quitting and Related Thoughts and Behaviors in a National Cohort of Aboriginal and Torres Strait Islander Smokers. Nicotine & Tobacco Research NTW396.
- Nicholson A, Borland R, Davey ME, Stevens M & Thomas DP 2015. Past quit attempts in a national sample of Aboriginal and Torres Strait Islander smokers. The Medical Journal of Australia 202.
- Noble N, Paul C, Sanson-Fisher R, Turon H, Turner N & Conigrave K 2016. Ready, set, go: a cross-sectional survey to understand priorities and preferences for multiple health behaviour change in a highly disadvantaged group. BMC health services research 16:488.
- Office on Smoking and Health (US) 2006. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. (ed., Centers for Disease Control and Prevention (US)). Atlanta: CDCP (US).
- Pan A, Wang YL, Talaei M, Hu FB & Wu TC 2015. Relation of active, passive, and quitting smoking with incident type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes & Endocrinology 3:958-67.
- Pircher SLM, Li SQ & Guthridge SL 2012. Trend analysis of hospital admissions attributable to tobacco smoking, Northern Territory Aboriginal and non-Aboriginal populations, 1998 to 2009. BMC Public Health 12:545-.
- PM&C (Department of the Prime Minister and Cabinet) 2019. Closing the Gap Report 2019. Canberra.
- Robertson J, Conigrave K, Ivers R, Hindmarsh E & Clough A 2013a. Addressing high rates of smoking in remote Aboriginal communities--new evidence for GPs. Australian Family Physician 42:492-6.
- Robertson J, Pointing BS, Stevenson L & Clough AR 2013b. "We Made the Rule, We Have to Stick to It": Towards Effective Management of Environmental Tobacco Smoke in Remote Australian Aboriginal Communities. International journal of environmental research and public health 10:4944-66.
- Sarin J, Hunt J, Ivers R & Smyth C 2015. Lifting the burden: a coordinated approach to action on Aboriginal tobacco resistance and control in NSW. Public Health Research & Practice 25:e2531528.
- Sawnani H, Jackson T, Murphy T, Beckerman R & Simakajornboon N 2004. The effect of maternal smoking on respiratory and arousal patterns in preterm infants during sleep. American Journal of Respiratory and Critical Care Medicine 169:733-8.
- Scollo M & Winstanley M 2019. Tobacco in Australia: Facts and issues. Melbourne: Cancer Council Victoria.
- Thomas DP, Davey ME, Viki L, Briggs VL & Ron BR 2015. Talking about the smokes: transforming the evidence to guide Aboriginal and Torres Strait Islander tobacco control. The Medical Journal of Australia 202.
- U.S. Department of Health and Human Services 2014. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
- Wang L, Mamudu HM, Alamian A, Anderson JL & Brooks B 2014. Independent and joint effects of prenatal maternal smoking and maternal exposure to second-hand smoke on the development of adolescent obesity: a longitudinal study. Journal of Paediatrics & Child Health 50:908-15.
- Zhang X, Condon JR, Rumbold A & Cunningham J 2011. Estimating cancer incidence in Indigenous Australians. Australian and New Zealand journal of public health 35:477-85.