
2. Demographic and social context
Aboriginal and Torres Strait Islander (First Nations) people are the first peoples of Australia. They are not one group but comprise hundreds of groups that have their own distinct set of languages, histories and cultural traditions.
In 2021, there were an estimated 984,000 First Nations people, representing 3.8% of the population (ABS 2021).
In 2021, about 3 in 5 (62%) First Nations people lived in New South Wales and Queensland.

339,710; 34.5% of the total First Nations population

273,119; 27.8%

120,006; 12.2%

76,487; 7.8%

78,696; 8.0%

52,069; 5.3%

33,857; 3.4%

9,525; 1.0%
Source: HPF Table D1 – AIHW analysis of Australian Bureau of Statistics (ABS) population estimates based on 2021 Census
First Nations people are more likely to live in urban and regional areas than remote areas, though the proportion of the total population of First Nations people is generally higher in more remote areas. In 2021:
- 84.6% (832,800 people) of First Nations people lived in non-remote areas: 40.8% lived in Major cities, 24.8% in Inner regional areas and 19.0% in Outer regional areas.
- Around 1 in 7 First Nations people (15.4% or 150,900 people) lived in Remote (6.0%) or Very remote areas (9.4%).
- The proportion of the total population in each area who were First Nations increased with remoteness, from 2.2% in Major cities, to 47.1% in Very remote areas (Table 2.1).
Table 2.1: First Nations population by remoteness area, 2021
|
Remoteness area |
Number |
Proportion (%) of total First Nations population |
Proportion (%) of total population of each area |
|---|---|---|---|
|
Major cities |
401,674 |
40.8 |
2.2 |
|
Inner regional |
244,012 |
24.8 |
5.3 |
|
Outer regional |
187,150 |
19.0 |
9.0 |
|
Remote |
58,727 |
6.0 |
19.6 |
|
Very remote |
92,146 |
9.4 |
47.1 |
Source: HPF Table D2 — AIHW analysis of ABS population estimates based on 2021 Census.
The First Nations population is relatively young (Figure 2.1). In 2021, one-half of First Nations people were aged under 24 years (median age), and about 1 in 3 (33.1%) First Nations people (about 325,800) were aged under 15, compared with fewer than 1 in 5 (17.9%) non-Indigenous Australians aged under 15.
Figure 2.1: Age structure of First Nations and non-Indigenous populations, 2021
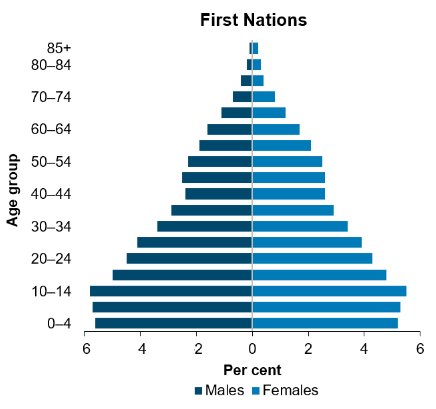
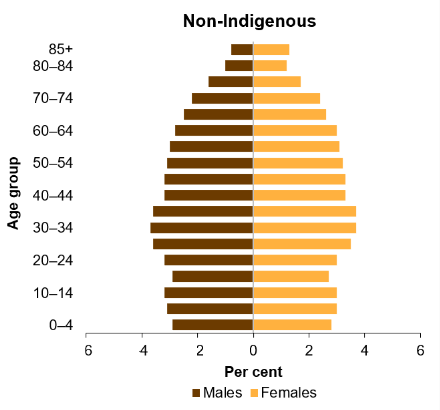
Source: HPF Table D3 – AIHW analysis of ABS population estimates based on 2021 Census.
Cultural and social determinants
There is evidence that cultural factors – Country and caring for Country, knowledge and beliefs, language, self-determination, family and kinship, and cultural expression – can be protective, and positively influence First Nations people’s health and wellbeing (Bourke et al. 2018).
The Mayi Kuwayu Study of Aboriginal and Torres Strait Islander Wellbeing aims to provide more evidence of how culture is related to First Nations people’s health and wellbeing (Australian National University 2020; Thurber et al 2022).
In contrast to cultural protective factors, racism or racial discrimination are associated with poorer physical and mental health (see, for example, Priest et al. 2011 and Paradies et al. 2014). Colonisation is recognised as having a fundamental impact on disadvantage and health among indigenous peoples worldwide, through social systems that maintain disparities (see, for example, Paradies & Cunningham 2012 and Paradies 2016).
Racism can be interpersonal (such as through exclusion, abuse, or stereotyping), or systemic (through policies, conditions, and practices).
Experiences of racism can have an impact on health through:
- reduced access to social resources, including employment, education, housing, health care, and other services
- psychological distress and increased likelihood of engaging in risk behaviours, such as substance use
- injury from assault (Paradies & Cunningham 2012).
Between March and May 2017, the Australian Government Department of Health, together with the Advisory Group on the Implementation Plan for the National Aboriginal and Torres Strait Islander Health Plan 2013-2023, led a consultation process (My life my lead) across Australia that examined the role of cultural and social factors on a person’s health and wellbeing. These consultations provided an opportunity for First Nations communities and leaders, governments, the non-government and private sectors to inform the National Aboriginal and Torres Strait Islander Health Plan 2021–2031 (released in December 2021).
Health is also influenced by social determinants – the circumstances in which people grow, live, work, and age (Commission on Social Determinants of Health 2008) – and individual health risk factors. Income, employment, and education are key social determinants of health that account for a large part of the disparity in First Nations and non-Indigenous health outcomes. Obesity and smoking are identified as the two most significant key health risk factors. Section 5 (Tier 2 – Determinants of Health) looks at these and other social determinants of health and risk factors.
Recent events
During 2020, 2 major events with global effects occurred – the COVID-19 (coronavirus disease 2019) pandemic, and the Black Lives Matter protests that followed the death of George Floyd, a 46-year-old African American man, during a police arrest in the United States.
The COVID-19 pandemic and response, and the Black Lives Matter protests, have highlighted recurring themes from First Nations health policy and research in Australia over the past 3 decades, including:
- continuing health inequalities between First Nations people and non-Indigenous Australians
- broader social inequalities between First Nations people and non-Indigenous Australians in areas that can affect health, including housing, education, employment, income, and access to adequate health care and other goods and services
- how well the health system serves the needs of First Nations people
- how governments can work in partnership and share decision-making with First Nations communities and leadership in identifying and responding to health priorities.
First Nations people remain at higher risk of experiencing more severe COVID-19 complications due to higher rates of pre-existing health conditions and challenges in accessing healthcare, particularly in remote areas. Between 2022 and March 2025 the age-standardised death rate from COVID-19 for First Nations people was 1.5 times the rate of non-Indigenous people (ABS 2025).
In Australia, 2020 also saw the signing of the National Agreement on Closing the Gap. This agreement is based on governments and First Nations people working in partnership and sharing decision-making to support better health and wellbeing outcomes among First Nations people.
More recently in 2023 and 2024, Australia has been experiencing high levels of inflation, with increased cost of living and higher interest rates impacting on housing costs and household disposable income (Reserve Bank of Australia 2024). Higher inflation has the potential to disproportionately impact the lowest income households and contribute to greater inequality, as lower income households spend a greater proportion of their income on essentials, tend to have fewer savings buffers, and have less scope to adjust spending patterns in response to rising costs (Wood et al. 2023).
On 14 October 2023, Australians voted in a referendum – the first of the 21st century – on whether to amend the Constitution to recognise Aboriginal and Torres Strait Islander peoples by establishing a body known as the Aboriginal and Torres Strait Islander Voice. The referendum did not pass.
The AIHW is committed to ensuring the National Agreement on Closing the Gap Priority Reforms are implemented in our approaches and processes. The AIHW will continue to produce data and information on the health and welfare of First Nations people, to inform policy, service delivery and community debate.