
Key facts
Why is it important?
Overweight and obesity is a global health problem and is associated with a significant reduction in life expectancy (OECD 2014; Peeters et al. 2003; Sevoyan et al. 2019). Overweight and obesity refers to abnormal or excessive fat accumulation that may impair health (WHO 2020). It typically arises from a sustained energy imbalance that occurs when energy intake through eating and drinking exceeds energy expended through physical activity (AIHW 2016a; Sevoyan et al. 2019). Being overweight or obese increases the risk of a range of health conditions, including coronary heart disease, type 2 diabetes, kidney and urinary diseases, some cancers, respiratory and joint problems, sleep disorders and social problems. Aboriginal and Torres Strait Islander people experience a disproportionately high rate of overweight and obesity.
Overweight and obesity is also associated with other health risk factors and social determinants of health. One example is prolonged financial stress, which is a predictor of obesity (see measure 2.08 Income) (Siahpush et al. 2014). Low income and food prices are associated with food security problems, and for these reasons, a nutritious diet is not always accessible for many Indigenous Australians (see measure 2.19 Dietary behaviours) (Markwick et al. 2014). Evidence also shows that incarceration is associated with weight gain and obesity in Indigenous youth (see measure 2.11 Contact with the criminal justice system) (Haysom et al. 2013). Other contributing factors include urbanisation, overcrowded housing and a lack of adequate access to health services (Sherriff et al. 2019).
Burden of disease
High body mass is a leading risk factor for poor health. High body mass was the second leading risk factor contributing to the health gap between Indigenous Australians and non-Indigenous Australians in 2011, accounting for 14% of the gap (AIHW 2016b, 2016c). High body mass contributed to 64% of the burden of diabetes for Indigenous Australians, 46% of the chronic kidney disease burden and 39% of the coronary heart disease burden. For risk factors such as high body mass that are becoming more common, current exposure may contribute to a higher disease burden in the future (AIHW 2016b).
Data findings
Overweight and obesity in those aged 15 and over
The 2018–19 National Aboriginal and Torres Strait Islander Health Survey (Health Survey) included height and weight measurements, to allow Body Mass Index (BMI) to be calculated. BMI is used to determine if a person is in a healthy weight range for their height. Where measurements were not taken, imputed values that were based on respondents with similar profiles were used to achieve estimates for the whole population.
In 2018–19, 71% (381,800) of Indigenous Australians aged 15 and over had a BMI in the overweight (25–29.9) or obese (>30.0) range (29% were overweight and 43% obese). A further 25% (133,500) had a BMI in the normal weight range (18.5–24.9) and 4% (20,800) were in the underweight category (<18.5).
After adjusting for differences in the age structure between the two populations, Indigenous Australians aged 15 and over were less likely than non-Indigenous Australians to be overweight (29% and 35%, respectively) but 1.5 times as likely to be obese (46% and 30%, respectively) (ABS 2019) (Figure 2.22.1).
Figure 2.22.1: Age-standardised proportion of persons aged 15 and over, by BMI category and Indigenous status, 2018–19
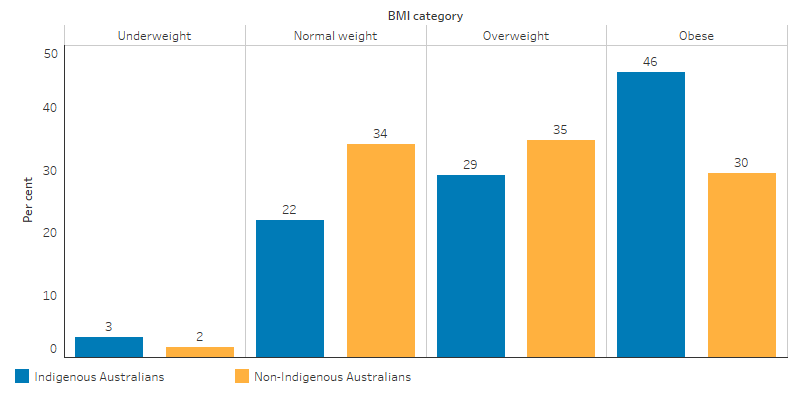
Source: National Aboriginal and Torres Strait Islander Survey 2018–19 (ABS Table 18.3).
Between the two periods 2012–13 and 2018–19, the proportion of Indigenous Australians aged 15 and over who were underweight remained the same (both 4%), of normal weight decreased from 31% to 25%, and overweight or obese increased from 66% to 71% (ABS 2013a, 2019) (Figure 2.22.2).
Figure 2.22.2: Proportion of Indigenous Australians aged 15 and over, by BMI category, 2012–13 and 2018–19
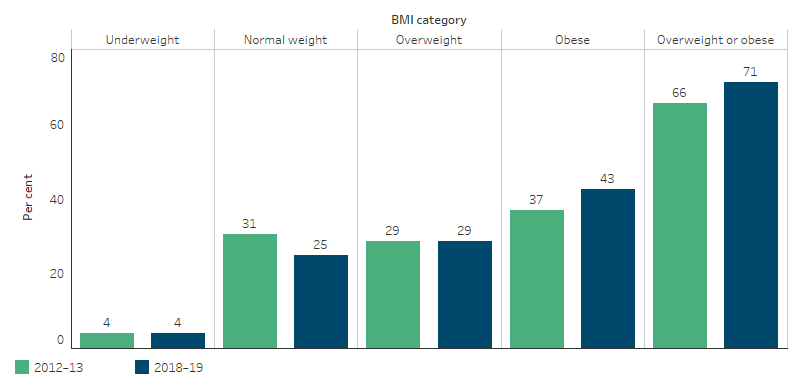
Source: Australian Aboriginal and Torres Strait Islander Health Survey 2012–13 (ABS Table 9.3); and National Aboriginal and Torres Strait Islander Health Survey 2018–19 (ABS Table 18.3).
Indigenous females were more likely to be obese than Indigenous males (45% compared with 40%, respectively), and less likely to be overweight than Indigenous males (27% compared with 31%, respectively) (ABS 2013b) (Figure 2.22.3).
Figure 2.22.3: Proportion of Indigenous Australians aged 15 and over, by BMI category and sex, 2018–19
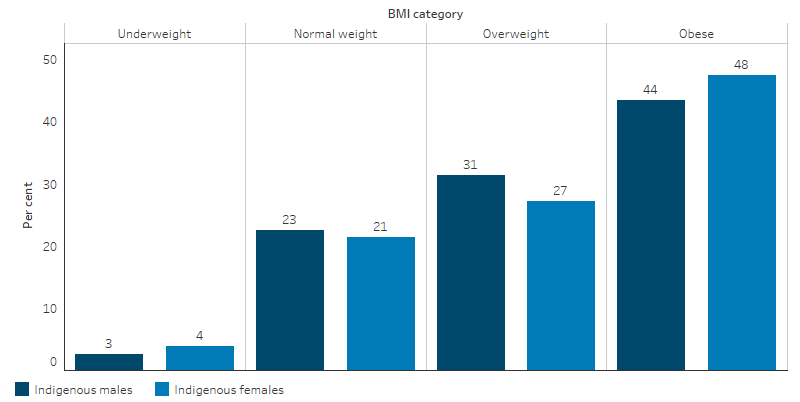
Source: National Aboriginal and Torres Strait Islander Survey 2018–19 (ABS Table 18.3).
Of Indigenous Australians aged 18 and over, 71% (345,500) had a waist circumference that increased their risk of developing chronic diseases (80cm or more for females and 94cm or more for males).
For Indigenous Australians with a BMI of overweight or obese, 87% (314,800) had a waist circumference that put them at increased risk of developing chronic diseases (95% or 178,700 for Indigenous females and 79% or 136,300 for males). For Indigenous Australians with a BMI of underweight or normal, 24% (30,600) had a waist circumference that put them at increased risk of developing chronic diseases (40% or 25,800 Indigenous females and 7.5% or 4,600 males) (ABS 2013b).
The proportion of the Indigenous population who had a BMI of overweight or obese increased with age, ranging from 42% for those aged 15–17 to 80%–82% for those aged over 35 (ABS 2013b) (Figure 2.22.4).
Figure 2.22.4: Proportion of Indigenous population overweight or obese, by age group, 2018–19
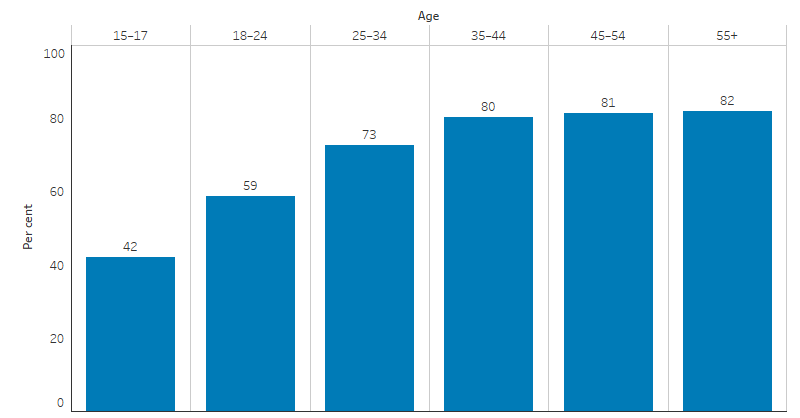
Source: National Aboriginal and Torres Strait Islander Survey 2018–19 (ABS Table 18.3).
The proportion of Indigenous Australians aged 15 and over who were obese in 2018–19 varied geographically. By remoteness, the proportion who were overweight or obese was highest in Inner regional areas (76%) and lowest in Very remote areas (62%) (ABS 2013b) (Figure 2.22.5).
Figure 2.22.5: Proportion of Indigenous population 15 and over who were overweight or obese, by remoteness, 2018–19
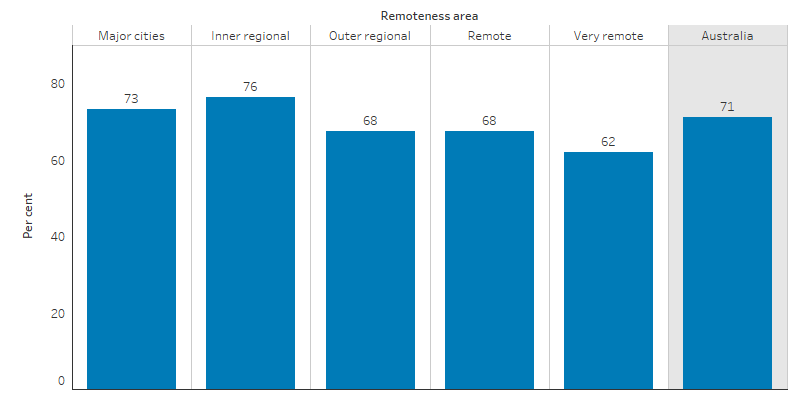
Source: National Aboriginal and Torres Strait Islander Survey 2018–19 (ABS Table 2.3).
The proportion of Indigenous Australians aged 15 and over who were overweight or obese was highest in Tasmania (76%) and lowest in the Northern Territory (59%) in 2018–19 (ABS 2013b) (Figure 2.22.6).
Figure 2.22.6: Proportion of Indigenous population 15 and over who were overweight or obese, by jurisdiction, 2018–19
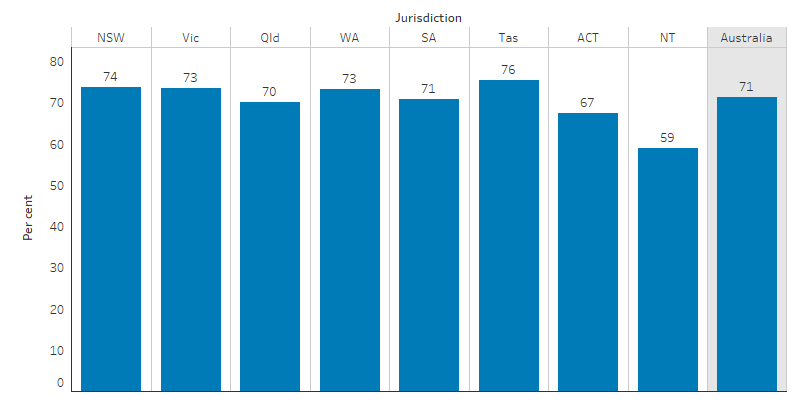
Source: National Aboriginal and Torres Strait Islander Survey 2018–19 (ABS Table 3.3).
The 2018–19 Health Survey showed that Indigenous Australians aged 18 and over who self-reported having diabetes were more likely to be obese than those who did not have diabetes (60% compared with 43%). Indigenous Australians with measured high blood pressure were more likely to be obese than those who did not have high blood pressure (58% compared with 41%) (Table D2.22.1).
Indigenous Australians who did not meet physical activity guidelines were more likely to be obese than those who met these guidelines (51% compared with 39%) (Table D2.22.2). Indigenous Australians who met daily vegetable intake guidelines were more likely to be obese than those who did not consume adequate daily vegetables (61% compared with 44%). Indigenous Australians who met daily fruit intake guidelines were slightly less likely to be obese than those who did not consume adequate daily fruit (42% compared with 47%) (Table D2.22.1).
Childhood weight
In 2018–19, Indigenous children aged 2–14 were underweight at a similar rate to non-Indigenous children (9% compared with 8%, respectively), were less likely to be in the normal weight range (54% compared with 67%), and more likely to be overweight or obese (37% compared with 25%) (Figure 2.22.7). The obesity rate for Indigenous children increased from the age of 2, with the highest rate at 14–17 years of age (16%) (ABS 2013b, 2018).
Figure 2.22.7: Proportion of children aged 2–14, by BMI category and Indigenous status, 2018–19
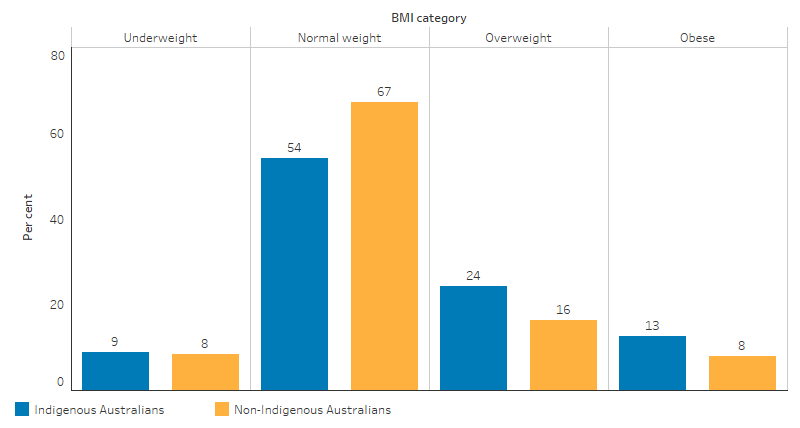
Source: National Aboriginal and Torres Strait Islander Survey 2018–19 (ABS Table 19.3) and National Health Survey 2017–18 (ABS Table 16.3).
Between the two periods 2012–13 and 2018–19, the proportion of Indigenous children aged 2–14 who were underweight remained similar (8% and 9%, respectively), of normal weight were 62% and 54%, respectively, and overweight or obese increased from 30% to 37% (ABS 2013a, 2019).
Indigenous primary health care clients
In December 2018, national data from 224 Commonwealth-funded Indigenous-specific primary health care organisations found that 27% (35,060) of regular clients aged 25 and over who had their BMI measured were overweight, and 44% (57,200) were obese. The proportion of clients who were obese was highest in Inner regional areas (49%) and Major cities (48%) and lowest in Very remote areas (38%) (Table D2.22.4).
Research and evaluation findings
Food insecurity (lack of access to affordable and nutritious food) can lead to obesity and malnutrition. Indigenous Australians experience food insecurity for many reasons, including low income, high food prices and limited availability of healthy foods where they live. Factors contributing to high food prices, particularly in remote areas, include freight charges and lack of competition. The combination of lower incomes with higher food prices means the proportion of income spent on food increases, making a healthier diet difficult to achieve for some Indigenous Australians. Research shows that the variety and quality of food in remote communities is also worse compared with cities (Davy 2016; Lee & Ride 2018).
Childhood is a critical period in which inequalities in health determinants such as socioeconomic status and overweight and obesity emerge (Jansen et al. 2013; Kim et al. 2017; Thurber et al. 2014). Indigenous children have higher rates of overweight and obesity than non-Indigenous children, placing them at an increased risk of metabolic disorders (including type 2 diabetes) earlier in life (Sherriff et al. 2019). A study in New South Wales showed that the rates of overweight and obesity has increased more rapidly in Indigenous than non-Indigenous school-aged children (Hardy et al. 2014). Research also shows that Indigenous children are at higher risk of developing early signs of kidney disease if they are overweight or obese, compared with non-Indigenous children (Kim et al. 2017). High BMI is found to be a predictor of short sleep duration and sleep apnoea for children, which impacts school performance (measure 2.04 Literacy and numeracy) and engagement in physical activity (measure 2.18 Physical activity) (Kassim et al. 2016; Magee et al. 2014).
There is international evidence that the consumption of sugar-sweetened drinks leads to weight gain. Indigenous Australian children consume higher quantities of soft drink per person compared with non-Indigenous children (Thurber et al. 2014). The odds of consuming sugar-sweetened drinks are significantly higher for Indigenous Australian children whose mothers have lower levels of education, experience housing instability, are living in urban areas and are living in disadvantaged neighbourhoods.
A recent study found that BMI showed a significant positive association with adverse cardio-metabolic profiles among Indigenous and non-Indigenous young adults. Adverse cardio-metabolic profiles were present in a large proportion of Indigenous participants, and remote Indigenous females had the highest predicted probability of having an adverse cardio-metabolic profile across all BMI categories (Sevoyan et al. 2019).
Go4Fun is a free program that operates in New South Wales for children aged 7–13 who are above a healthy weight. The government-funded program operates for 10 weeks during the school term and is run by qualified health professionals including dietitians and physiologists. Between 2009 and 2012, almost 6% of the program’s participants were Indigenous. An evaluation of the program showed that Indigenous children were less likely to complete the program and highlighted the need for stronger engagement with the Indigenous community to develop more culturally appropriate strategies (Welsby et al. 2014).
The School Nutrition Projects (SNP) were introduced in the Northern Territory as part of the Australian Government’s 2007 Northern Territory Emergency Response (NTER). In 2016, an evaluation of aspects of the SNP investigated the dietary requirements of students in remote Indigenous schools, enablers and barriers to program delivery, and students’ nutrition during school holiday periods. The SNP was found to provide an important part of the daily diet of students, and the majority of food and beverages provided were healthy, with fruit and vegetables dominating. However, some food and beverages were considered discretionary, and it was suggested that minimising the inclusion of these would help achieve total saturated fat and sodium intake closer to the World Health Organization recommendations (Menzies School of Health Research 2017).
The Deadly Choices program is a school-based chronic disease and education program that encourages young people to be positive role models in reshaping health, lifestyle and physical activity choices. An evaluation of the program found promising results in physical activity, breakfast intake, and fruit and vegetable consumption, all of which are core components of healthy weight management (Malseed et al. 2014).
An evaluation of the community-led healthy lifestyle program ‘Knockout Health Challenge’ in New South Wales found the program was effective in reducing weight and in the promotion of healthy lifestyles among Indigenous Australians. At the end of the challenge participants were more physically active and had increased fruit and vegetable consumption. Participants identified other positive health outcomes such as improved wellbeing, reduced anxiety and stress, increased community awareness of healthy lifestyles, and increased community pride and connectedness. Men were less likely to participate than women and were less likely to reduce their BMI during the challenge, suggesting that further research is needed regarding how to engage men in healthy lifestyle interventions (Passmore et al. 2017).
Implications
Given the health risks associated with being obese or overweight, the high rate for Indigenous Australians requires urgent attention. It is second only to tobacco use in terms of the contribution of modifiable risk factors to the health gap experienced by Indigenous Australians (AIHW 2016b).
The reversal of obesity is difficult even in the absence of environmental and social barriers. Therefore, early intervention to prevent the onset of excessive weight gain is likely to be the most effective strategy (Thurber et al. 2014). Studies reporting success in reducing obesity have a number of common characteristics, including a focus on physical activity and diet as opposed to diet alone, the ability to accommodate the preferences of participants, a group focus, and choice between several physical activities. Programs must also be culturally acceptable, conveniently located, easily incorporated into the daily schedule and show goal attainment that is realistic and appropriate (Canuto et al. 2011).
There is evidence that health programs and policies lead to greater outcomes when they are created with the intended participants. Indigenous Australians should be engaged in the development of any strategies to ensure they are culturally relevant (Schwarzman et al. 2019) (Sevoyan et al. 2019). The Knockout Health Challenge is a good example that was led by Indigenous communities and with community engagement in the program design and implementation. The program was also flexible to adapt to local needs and priorities (Passmore et al. 2017).
It will be important for strategies and policies to address the broader structural determinants of health inequalities, for example, lack of access to adequate housing, healthy food and opportunities to participate in physical activities (Sevoyan et al. 2019). Interventions to improve food security should consider education programs, price caps and subsidies to stores and consumers.
A recent review of evaluation methods and quality in Australian health promotion agencies also highlighted the importance of improving the quality of evaluations in health promotion and preventive health to help build the evidence base for prevention strategies (Schwarzman et al. 2019).
The policy context is at Policies and strategies.
References
- ABS (Australian Bureau of Statistics) 2013a. Australian Aboriginal and Torres Strait Islander Health Survey: First Results Australia 2012–13. cat. no. 4727.0.55.001. Canberra: AIHW.
- ABS 2013b. Australian Aboriginal and Torres Strait Islander Health Survey: Updated Results 2012–13. Cat. no. 4727.0.55.006. Canberra: ABS.
- ABS 2018. National health survey: First results, 2017–18.
- ABS 2019. National Aboriginal and Torres Strait Islander Health Survey, 2018–19. 4715.0. Canberra: ABS.
- AIHW (Australian Institute of Health and Welfare) 2016a. Australia's health 2016. Canberra: AIHW.
- AIHW 2016b. Australian Burden of Disease Study 2011: impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2011. Canberra: AIHW.
- AIHW 2016c. Australian Burden of Disease Study: impact and causes of illness and death in Australia 2011. Canberra: AIHW.
- Canuto KJ, McDermott RA, Cargo M & Esterman AJ 2011. Study protocol: a pragmatic randomised controlled trial of a 12-week physical activity and nutritional education program for overweight Aboriginal and Torres Strait Islander women. BMC Public Health 11:655.
- Davy D 2016. Australia’s Efforts to Improve Food Security for Aboriginal and Torres Strait Islander Peoples. Health and Human Rights 18:209.
- Hardy LL, O'Hara BJ, Hector D, Engelen L & Eades SJ 2014. Temporal trends in weight and current weight-related behaviour of Australian Aboriginal school-aged children. The Medical Journal of Australia 200:667-71.
- Haysom L, Indig D, Moore E, Hardy LL & van den Dolder PA 2013. Prevalence and perceptions of overweight and obesity in Aboriginal and non-Aboriginal young people in custody. The Medical Journal of Australia 199:266-70.
- Jansen PW, Mensah FK, Nicholson JM & Wake M 2013. Family and neighbourhood socioeconomic inequalities in childhood trajectories of BMI and overweight: longitudinal study of Australian children. PloS one 8:e69676.
- Kassim R, Harris M-A, Leong GM & Heussler H 2016. Obstructive sleep apnoea in children with obesity. Journal of Paediatrics & Child Health 52:284-90.
- Kim S, Macaskill P, Hodson EM, Daylight J, Williams R, Kearns R et al. 2017. Beginning the trajectory to ESKD in adult life: albuminuria in Australian aboriginal children and adolescents. Pediatric Nephrology 32:119-29.
- Lee A & Ride K 2018. Review of nutrition among Aboriginal and Torres Strait Islander people. Australian Indigenous HealthInfoNet.
- Magee C, Caputi P & Iverson D 2014. Lack of sleep could increase obesity in children and too much television could be partly to blame. Acta Paediatrica 103:e27-31.
- Malseed C, Nelson A & Ware R 2014. Evaluation of a School-Based Health Education Program for Urban Indigenous Young People in Australia. Health:587-97.
- Markwick A, Ansari Z, Sullivan M & McNeil J 2014. Social determinants and lifestyle risk factors only partially explain the higher prevalence of food insecurity among Aboriginal and Torres Strait Islanders in the Australian state of Victoria: a cross-sectional study. BMC Public Health 14:598.
- Menzies School of Health Research 2017. An Evaluation of the School Nutrition Projects in the Northern Territory Final Report. Department of the Prime Minister & Cabinet.
- OECD (Organisation for Economic Co-operation and Development) 2014. Obesity Update. OECD Publishing.
- Passmore E, Shepherd B, Milat A, Maher L, Hennessey K, Havrlant R et al. 2017. The impact of a community-led program promoting weight loss and healthy living in Aboriginal communities: the New South Wales Knockout Health Challenge. BMC Public Health 17:951.
- Peeters A, Barendregt JJ, Willekens F, Mackenbach JP, Mamun AA & Bonneux L 2003. Obesity in adulthood and its consequences for life expectancy: a life-table analysis. Annals of Internal Medicine 138:24-32.
- Schwarzman J, Nau T, Bauman A, Gabbe BJ, Rissel C, Shilton T et al. 2019. An assessment of program evaluation methods and quality in Australian prevention agencies. Health Promotion Journal of Australia.
- Sevoyan A, Davison B, Rumbold A, Moore V & Singh G 2019. Examining the relationship between body mass index and adverse cardio-metabolic profiles among Australian Indigenous and non-Indigenous young adults. Scientific reports 9:1-8.
- Sherriff SL, Baur LA, Lambert MG, Dickson ML, Eades SJ & Muthayya S 2019. Aboriginal childhood overweight and obesity: the need for Aboriginal designed and led initiatives.
- Siahpush M, Huang TT, Sikora A, Tibbits M, Shaikh RA & Singh GK 2014. Prolonged financial stress predicts subsequent obesity: results from a prospective study of an Australian national sample. Obesity (Silver Spring) 22:616-21.
- Thurber K, Boxall A & Partel K 2014. Overweight and obesity among Indigenous children: individual and social determinants. Canberra: AHHA.
- Welsby D, Nguyen B, O’Hara BJ, Innes-Hughes C, Bauman A & Hardy LL 2014. Process evaluation of an up-scaled community based child obesity treatment program: NSW Go4Fun®. BMC Public Health 14:140.
- WHO (World Health Organisation) 2020. Obesity and overweight. Viewed 15 July 2020.