
Key messages
- From July 2017 to June 2019, 99.2% (958,443) of hospitalisations in public hospitals for Aboriginal and Torres Strait Islander people occurred in accredited hospitals, compared with 99.0% for non-Indigenous Australians.
- From July 2017 to June 2019, all hospitalisations for Indigenous Australians in public hospitals in Outer regional and Very remote areas occurred in accredited hospitals. Nearly all hospitalisations in Inner regional and Remote areas occurred in accredited hospitals (both 99.9%), whilst in Major cities, 97.5% occurred in accredited hospitals.
- About 96% of general practices registered with Australian General Practice Accreditation Limited (AGPAL), Quality Practice Accreditation (QPA) or Australian Council on Healthcare Standards (ACHS) were fully accredited by the respective organisation in 2019.
- According to the 2017–18 Online Services Report, of the 198 Commonwealth funded Indigenous primary health care organisations, 171 employed a general practitioner (85% with accreditation). Of the 140 Aboriginal and Community Controlled Health Organisations, 133 employed a general practitioner.
Why is it important?
Accreditation is a process through which a recognised external body assesses the extent to which a health care organisation meets applicable quality standards. Quality standards typically address issues that present a significant risk of harm to patients and may include topics such as clinical governance, infection control, medication safety, comprehensive care, communicating for safety, recognising and responding to patient deterioration. Assessments of quality often result in recommendations for action. Accreditation is one way to contribute to accountability, because it aims to ensure a level of competence and has the potential to improve the quality of services (Farquhar 2017).
The services accessed by Aboriginal and Torres Strait Islander people should be able to demonstrate compliance with requirements in the National Safety and Quality Health Service (NSQHS) Standards, some of which include specific actions relating to Aboriginal and Torres Strait Islander peoples to achieve accreditation. Accreditation provides one measure of the capability of services, based on their skills and knowledge, to provide quality health services to Indigenous Australians.
In Australia, there are accreditation systems for both hospitals and general practice. All public and private hospitals, day procedure services and public dental practices are required to be accredited to the NSQHS Standards. There are six accrediting agencies approved by the Australian Commission on Safety and Quality in Health Care (ACSQHC) to assess against the eight NSQHS Standards (ACSQHC 2017).
The NSQHS Standards were released in 2017 and assessments began in January 2019. Six Indigenous specific actions were implemented in the Standards that aim to meet the needs of Indigenous Australian patients. These include actions aimed at improving the cultural competency and cultural awareness of the workforce, recognising the importance of cultural beliefs and practices, and better identification and recording of Indigenous Australians (ACSQHC 2017).
In 2021 the NSQHS Preventing and Controlling Infections Standard was updated. The changes took into consideration lessons learned from the response to SARS-CoV 2 (COVID-19). The changes aim to help health service organisations prevent, control and respond to infections that lead to outbreaks, epidemics or pandemics (ACSQHC 2021).
In general practice, accreditation involves assessment against standards set by the Royal Australian College of General Practitioners (RACGP) that have been grouped into three key modules: the core module; the quality improvement module; and the General Practice module (RACGP 2017). The standards are based on the best available evidence of how general practices can provide safe and quality healthcare. In order for a practice to be accredited against the standards, it must be formally assessed by an approved accrediting agency (RACGP 2017).
The ACSQHC coordinates the National General Practice Accreditation Scheme. As part of the Scheme, ACSQHC approves accrediting agencies to assess services according to the RACGP Standards for General Practices. As at 1 January 2020, there are five approved providers: Australian General Practice Accreditation Limited (AGPAL), Quality Practice Accreditation (QPA), the Australian Council on Health-care Standards (ACHS), Global-Mark and the Institute for Healthy Communities Australia Certification (IHCAC) (ACSQHC 2021).
Data findings
Hospitalisations in accredited hospitals
From July 2017 to June 2019, 99.2% (958,443) of hospitalisations for Indigenous Australians in public hospitals occurred in accredited hospitals, with the remaining 0.8% of hospitalisations occurring in non-accredited hospitals or those where accreditation status was unknown (338 and 7,533 hospitalisations respectively). The proportion of hospitalisations in public hospitals for non-Indigenous Australians that occurred in accredited hospitals was 99.0% (Table D3.19.1).
All hospitalisations for Indigenous Australians in public hospitals in Outer regional and Very remote areas occurred in accredited hospitals. Nearly all hospitalisations in public hospitals for Indigenous Australians in Inner regional and Remote areas occurred in accredited hospitals (both 99.9%). In Major cities, this proportion was 97.5% (Table D3.19.3, Figure 3.19.1).
Figure 3.19.1: Public hospitalisations in accredited hospitals, by Indigenous status and remoteness, Australia, July 2017 to June 2019
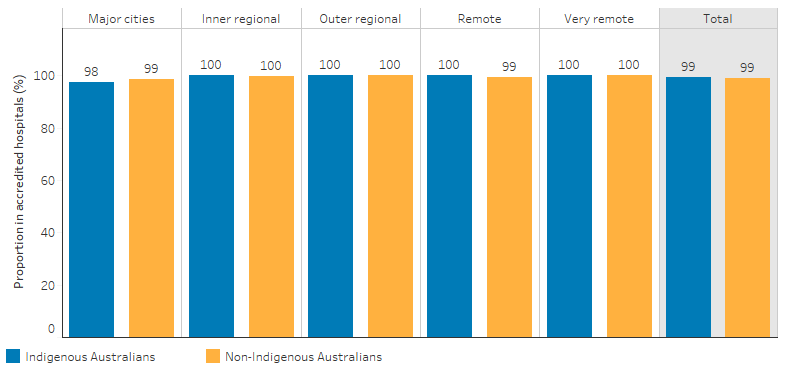
Note: Information on hospital accreditation reported here may not be consistent with data reported by the Australian Commission on Safety on Quality in Health Care and is not comparable across jurisdictions.
Source: Table D3.19.3. AIHW analysis of National Hospital Morbidity Database and National Public Hospitals Establishment Database.
All hospitalisations in public hospitals for Indigenous Australians living in Victoria, South Australia, Australian Capital Territory and Northern Territory occurred in an accredited public hospital. For Indigenous patients in Western Australia and New South Wales, about 0.2% (777 patient days) and 0.5% (3,327 patient days) of hospitalisations in public hospitals were in non-accredited hospitals, respectively (Table D3.19.2).
Accreditation of general practices
In 2019, 96% (6,185) of general practices registered with one of three organisations for which data is available—Australian General Practice Accreditation Limited (AGPAL), Quality Practice Accreditation (QPA) or Australian Council on Healthcare Standards (ACHS)—were fully accredited by the respective organisation.
When these general practices are disaggregated into six categories representing the proportion of the Indigenous population in the Primary Health Network they service, the rate of accreditation was lowest in areas where Indigenous Australians make up 10% or more of the population (94%). However, rates of accreditation of general practices were similar in all Indigenous population size categories (Table D3.19.5, Figure 3.19.2).
Figure 3.19.2: Proportion of general practices registered for accreditation through AGPAL, QPA or ACHS that had been accredited, by per cent of the population that is Indigenous, 2019
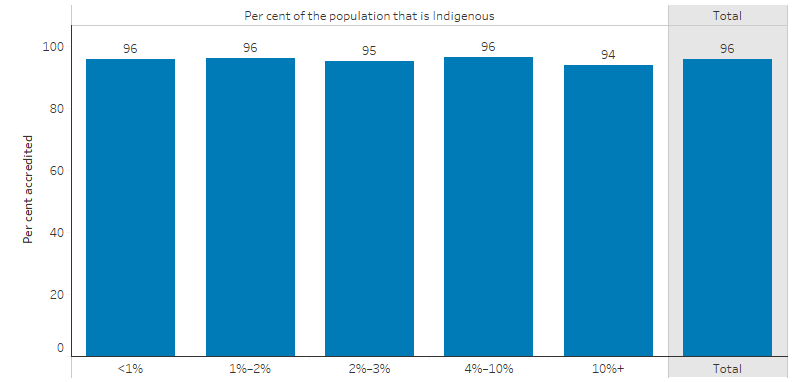
Source: Table D3.19.5. AIHW analysis of Australian General Practice Accreditation Limited (AGPAL) and Quality Practice Accreditation (QPA) data (as at 30 June 2019) and the Australian Council on Healthcare Standards (ACHS) data (as at September 2019).
Accreditation of primary health care organisations
The 2017–18 Online Services Report data collection includes data on the accreditation status of Commonwealth-funded Indigenous primary health care organisations.
Of the 198 Commonwealth funded primary health care organisations:
- 171 employed a general practitioner (GP)
- 85% of these reported having a current clinical Royal Australian College of General Practitioners (RACGP) and/or organisational accreditation
- 140 were Aboriginal and Community Controlled Health Organisations (ACCHO), of which 133 employed a GP
- 98% reported having a current clinical RACGP and or organisational accreditation (Table D3.19.6, Figure 3.19.3).
Figure 3.19.3: Proportion of Commonwealth-funded Indigenous primary health care organisations, by accreditation status and presence of general practitioner, 2017–18
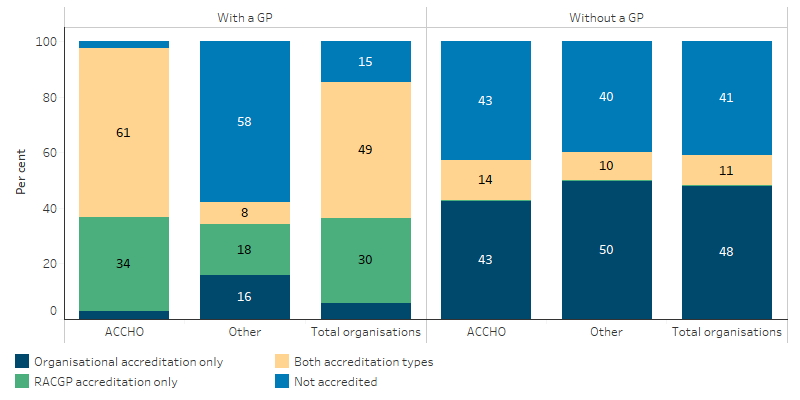
Source: Table D3.19.6. AIHW analyses of Online Services Report data collection, 2017–18.
Research and evaluation findings
A review by Leggat and others (2017) examined health service quality system implementation in eight Australian public hospitals using document review, self-evaluation, and qualitative data from interviews and focus groups. The study found that in the absence of an agreed purpose for the quality system, quality of care was something that was largely compliance based and seen as an extra set of tasks to do, rather than as a contribution to safe and high-quality care. Participants in focus groups complained about the burden of quality and safety paperwork, and quality systems were described as focusing more on process than people. The study concluded that quality systems focus primarily on compliance and finding errors and don’t contribute to consistent high quality care (Leggat & Balding 2017).
Greenfield and others (2019) conducted research into whether longitudinal participation in an accreditation program translates into improvement in continuity of quality patient care and human resource management (HRM) processes outcomes. A score for HRM processes was constructed using five accreditation criteria items: HRM planning; recruitment and selection; training and development; performance management; and support services. There were 311 Australian hospitals included in the study. Results show that accreditation is an important external driver that contributes to continual and systematic quality improvement changes in safety, quality and effectiveness of health organisations (Greenfield et al. 2019).
On the other hand, a systematic review of accreditation found no evidence to support accreditation and/or certification being linked to measurable changes in quality of care. Accreditation requires substantial investment and distracts staff from their primary clinical goals. The review also found, however, that there are challenges in measuring accreditation and certification (Brubakk et al. 2015). International research by Grepperud (2015) found that hospital accreditation may not be socially efficient, and that there is insufficient evidence to show that accreditation leads to quality improvements in hospitals (Grepperud 2015).
A recent report by the Grattan Institute (2018) suggests Australia’s hospital accreditation system is not good enough and that there is large variation across Australia. The authors point out that major safety failures in Australian hospitals in recent decades have all occurred in hospitals that passed accreditation. The paper argues that there is limited evidence to show accreditation improves patient outcomes and that the standards hospitals are assessed against lack a strong evidence base. Even with the revised accreditation system that came into effect in January 2019, authors recommend that the accreditation system needs an overhaul. They propose a new model that focuses on local patient outcomes and improvement, rather than processes and compliance with minimum standards (Duckett & Jorm 2018).
With the development of the second edition of the NSQHS Standards, the ACSQHC conducted a review to identify improvements to the assessment process, to be phased in with the updated standards from January 2019 (ACSQHC 2018a). The 2018 review of the Australian Health Service Safety and Quality Accreditation Scheme (AHSSQA Scheme) proposed strategies and sub-strategies aimed at improving the reliability of the accreditation process (ACSQHC 2018b). The six identified strategies were designed to ensure that the process of accreditation will accurately assess compliance against the NSQHS Standards rather than examine their preparedness for an assessment. Proposed strategies included:
- Improve the veracity of health service organisation assessments.
- Improve the effectiveness and expertise of the assessment team.
- Assess the health service organisation’s safety and quality data to better inform assessment processes.
- Improve regulatory oversight.
- Improve communications about the assessments and their outcomes.
- Improve resources and support for health service organisations.
In 2021, the Australian Medical Council began a process to review its accreditation standards, with a focus to improve safety, quality and experience of care for Indigenous patients. In particular, Action 1.21 of the NSQHS Standards suggests strengthening cultural competence of health staff through high-quality cultural safety training. A national survey was conducted in the same year to estimate the coverage and the quality of cultural safety training programs in both public and private health service organisations across Australia. A total of 421 responses were collected from participants representing 6 service types: public hospitals, private hospitals, community health services, day procedure services, mental health services and public health departments. When asked “Who leads/facilitates the delivery of the training?”, about 53% of the training was reported to be fully or partly delivered by an Indigenous member of the workforce. The number and duration of the training sessions varied greatly. Critically, only 21% of respondents reported their training had been evaluated (out of the 274 responses to the question “Has this health service organisation evaluated the impact of cultural safety training?”). The report concluded that the effectiveness of cultural safety training has not been systematically assessed. The current training focused more on knowledge, attitudes and understanding rather than how to ensure health services provide patient-centred, culturally safe health care (Hunter et al. 2022).
The emphasis of patient-centred service is consistent with a systematic meta-ethnography review that has characterised the 4 elements contributing to culturally safe clinical practice for Indigenous populations: personable two-way communication; well-resourced Indigenous health workforce; trusting relationships between clinicians and their Indigenous patients; and supportive health care systems. These elements were inter-related which centred around a health care system that cultivates a culturally capable workforce. That included cross-cultural training for health staff and increasing workforce representation by Indigenous health staff. In the context that Indigenous patients frequently experienced discrimination, miscommunications and cultural dissonance which are common barriers for treatment seeking and continuity of care, a respective and culturally supportive clinical environment was highly valued by Indigenous patients and their families (De Zilva et al. 2021).
Implications
A recent evidence brief exploring the value of accreditation to health systems and organisations considers the research into health services accreditation to be lacking. The requirement in Australia that all health facilities be accredited also prevents comparisons between accredited and non-accredited facilities and the research therefore is mostly observational studies. The brief suggests that any policy decisions relating to accreditation should consider that health care is constantly changing and adapting to changes in population, technology and new research, and that accreditation should also be flexible and responsive. Culture and leadership are positively associated with accreditation, and ensuring staff value accreditation can help to support a culture of safety and quality in health services (Swiers & Haddock 2019).
It has been suggested that the focus of accreditation should shift from compliance based to outcomes and improvement, and more engagement should occur with hospitals to support them in improving. Accreditation should be used as a tool for a health organisation’s continuous improvement, rather than a point in time occurrence. Accreditation should also be based on measurable outcomes and tailored to individual health services (Duckett & Jorm 2018).
Evaluations of the accreditation process in Australia and internationally are lacking and strategies identified in the review of the AHSSQA Scheme will require evaluation in order to provide evidence of the value of accreditation to health organisations (Swiers & Haddock 2019). This should include evaluating the six actions in the NSQHS Standards that focus specifically on meeting the needs of Indigenous Australians, and are aimed at improving identification of Indigenous status and ensuring care is culturally safe.
For Commonwealth-funded Indigenous primary health care, almost all Aboriginal Community Controlled Health Organisations had a current clinical RACGP and or organisational accreditation. The data suggests that some services are not accredited and these were more likely not to be community controlled.
The adoption of the national Key Performance Indicators by Commonwealth-funded Indigenous primary health care is a demonstration of the commitment to continuous quality improvement practices to deliver high quality care to Indigenous Australians. This serves as an example to mainstream primary care services that deliver care to Indigenous Australians.
The Australian Government is developing a National Primary Health Care Data Collection (the Data Collection). The Data Collection will fill data and information gaps in relation to primary health care data for population health monitoring, research, policy, and planning. The project is currently in the development phase, following an extensive consultation process that took place in 2018-2020. Consultations revealed the importance of Indigenous status identification and an opportunity, once the asset is developed, for mainstream data to be compared with Indigenous specific primary health care services. This will allow for assessment of the quality of mainstream primary health care in delivering services to Indigenous Australians (AIHW 2019).
References
- ACSQHC (Australian Commission on Safety and Quality in Health Care) 2017. National Safety and Quality Health Service Standards (Second Edition). Sydney, Australia: ACSQHC.
- ACSQHC 2018a. Review of hospital accreditation further embeds safety improvements in the Australian health care sector.
- ACSQHC 2018b. Review of the Australian Health Service Safety and Quality Accreditation Scheme: Improving the reliability of health service organisation accreditation processes. Sydney.
-
ACSQHC 2021. National Safety and Quality Health Service Standards. 2nd ed. – version 2. Sydney: ACSQHC; 2021.
- AIHW (Australian Institute of Health and Welfare) 2019. Developing a National Primary Health Care Data Asset: consultation report. Canberra: AIHW.
- Brubakk K, Vist GE, Bukholm G, Barach P & Tjomsland O 2015. A systematic review of hospital accreditation: the challenges of measuring complex intervention effects. BMC health services research 15:1-10.
-
De Zilva S, Walker T, Palermo C & Brimblecombe J 2021. Culturally safe health care practice for Indigenous Peoples in Australia: A systematic meta-ethnographic review. Journal of Helath Services Research & Policy 27:74-84.
- Duckett S & Jorm C 2018. Safer care saves money: how to improve patient care and save public money at the same time. Grattan Institute.
- Farquhar M 2017. Why Accreditation Must Evolve to Determine Accountability and Quality in Healthcare. URAC.
- Greenfield D, Lawrence S, Kellner A, Townsend K & Wilkinson A 2019. Health service accreditation stimulating change in clinical care and human resource management processes: A study of 311 Australian hospitals. Health Policy 123:661-5.
- Grepperud S 2015. Is the hospital decision to seek accreditation an effective one? The International journal of health planning and management 30:E56-E68.
- Leggat SG & Balding C 2017. A qualitative study on the implementation of quality systems in Australian hospitals. Health services management research 30:179-86.
- RACGP (The Royal Australian College of General Practitioners) 2017. Standards for general practices (5th Edition). East Melbourne, Vic.
- Swiers R & Haddock R 2019. Assessing the value of accreditation to health systems and organisations. Deeble Institute for Health Policy Research, Australian Hospital and Healthcare Association.