
In 2017, the two most common drugs detected in Indigenous prison detainees were cannabis and methamphetamine
In 2014–15, 17% of Indigenous Australians aged 15 and over reported drug-related problems as a cause of stress in their lives
Key messages
- In 2018−19, 29% of Aboriginal and Torres Strait Islander people aged 15 and over reported having used substances in the previous 12 months, up from 23% in 2008.
- In 2018−19, Indigenous males aged 15 and over had higher rates of recent substance use than Indigenous females (37% compared with 22%).
- In 2018–19, for Indigenous Australians aged 15 and over, those who used substances were more likely than those who did not use substances to be a current smoker (62% compared with 36%, respectively) and to drink at levels exceeding the single occasion risk (72% compared with 49%, respectively).
- From 2008 to 2018−19, the proportion of Indigenous Australians who reported using marijuana, hashish or cannabis resin increased from 14% to 25% in remote areas and from 18% to 24% in non-remote
- Marijuana, hashish or cannabis resin were the most common illicit substances used in the last 12 months among Indigenous Australians aged 15 and over (used by around 104,600 people, or 25% of those aged 15 and over), in 2018−19.
- Of drug-related hospitalisations of Indigenous Australians between July 2017 and June 2019, 59% were due to mental/behavioural disorders (7,370 hospitalisations), 39% due to poisoning (4,828 hospitalisations), and 2% due to other direct harm.
- The age-standardised rate of hospitalisations related to drug use for Indigenous Australians increased from 3.4 to 8.1 per 1,000 population (an estimated 144% or nearly a 2.5-fold increase based on linear regression analysis) over the decade from 2009–10 and 2018–19.
- Of Indigenous patients hospitalised for drug use between July 2017 and June 2019, 59% (7,370) were due to mental/behavioural disorders caused by the use of substances, poisoning accounted for 39% (4,828 hospitalisations) and 2% due to other direct harm.
- Methamphetamines was the most common drug type for drug-related hospitalisations among Indigenous Australians, accounting for one-fourth (25% or 3,126 hospitalisations) of these hospitalisations.
- There was a rise in the use of painkillers or analgesics for non-medical purposes by Indigenous Australians between 2008 and 2014–15 (from 5% to 12%), but the proportion was down to 3% in 2018–19. This aligns with codeine being made a prescription-only medication from 1 February 2018.
- An evaluation of a culturally adapted mixed-methods intervention to address chronic mental illness and comorbid substance use in remote Indigenous communities suggested that brief interventions that address co-morbid disorders in an integrated way can result in significant change in substance use and improved mental health outcomes.
- Since the rollout of Low Aromatic Fuel (LAF) in place of regular unleaded petrol by the Australian Government in 2005, among 11 Indigenous communities who have been surveyed, the total number of people sniffing petrol declined by 95% from 453 to 22 cases between 2006 and 2018.
- Research has also shown that the availability and use of youth engagement activities, such as sport and recreation in communities is an important influence on reducing the demand for petrol and other volatile substances among young people.
Why is it important?
Drug and other substance use is a contributing factor to illness and disease, accident and injury, violence and crime, family and social disruption, education and workplace problems (SCRGSP 2014). Illicit drug use encompasses a range of categories including the use of illegal drugs, inappropriate pharmaceutical use, and use of psychoactive substances (including inhalants) (AIHW 2018).
Substance use is associated with mental health problems (Catto & Thomson 2008) and has been found to be a factor in suicides (Robinson et al. 2011). A recent study of Indigenous and non-Indigenous hospitalisations for suicidal ideation and self-harm, found that a higher proportion of Indigenous patients had diagnoses of substance use disorders than non-Indigenous patients (Leckning, et al. 2022). In 2014–15, of Indigenous Australians with a mental health condition, around two in five had used substances in the last 12 months (ABS 2016).
The use of drugs or other substances including inhalants is linked to various other medical conditions. Injecting drug users, for example, have an increased risk of contracting blood-borne viruses such as hepatitis or HIV (Kratzmann et al. 2011) and around half of heroin and opioid users report overdosing (Catto & Thomson 2008). Risky sexual behaviour is associated with alcohol and illicit drug use, leading to increased sexually transmitted infections (STIs) among younger people (Wand et al. 2016).
For communities, there is increased potential for social disruption, such as that caused by domestic violence, crime and assaults. Drugs and other substance use play a significant role in Indigenous Australians’ involvement in the criminal justice system (see measure 2.11 Contact with the criminal justice system).
Volatile substance use, including petrol sniffing and inhalation of products such as aerosol deodorants, spray paints and glue, is difficult to control because the active substances are found in many common products that have legitimate uses. Common inhalants are legal, readily available, and inexpensive substances. People who use these products as inhalants risk sudden death, long-term health problems and continued use can also lead to the social alienation of those who sniff, violence and reduced self-esteem (Karam et al. 2014; Midford et al. 2011). There is little information on petrol sniffing in the established datasets used in this report. However, it is covered in more detail in the section on research and evaluations.
Burden of disease
In 2018, there were an estimated 16,645 years of healthy life lost by Indigenous Australians (disease burden, DALY) were attributable to illicit drug use (6.9% of the total disease burden) for Indigenous Australians, corresponding to a rate of 23 years of healthy life lost per 1,000 population. Illicit drug use was responsible for a higher proportion of the fatal burden (8.9%, or 10,145 years of life lost) than non-fatal burden (5.1%, or 6,500 years of life lived with disability).
Illicit drug use was the second leading risk factor contributing to the total burden for Indigenous Australians aged between 15–24 (accounting for 13% of the total burden, or 3,698 disability adjusted life years) and 25–44 years (13% of the total burden, or 9,192 disability adjusted life years). The drugs contributing most to the burden due to illicit drug use were opioids (31% of illicit drug use burden, 5,207 DALY), amphetamines (27%, 4,487 DALY) and cannabis (23%, 3,934 DALY), which collectively accounted for around four-fifths (82%) of the disease burden attributable to illicit drug use. After adjusting for the difference in the age-structure between Indigenous and non-Indigenous populations, the total burden attributable to illicit drug use was 3.7 times as high for Indigenous Australians as for non-Indigenous Australians, and accounted for 7.4% of the total health gap (AIHW 2022).
Data findings
Reported data on substance use are reported in the 2018–19 National Aboriginal and Torres Strait Islander Health Survey. In 2018–19, 29% (123,319) of Indigenous Australians aged 15 and over reported that they had used drugs or other substances in the previous 12 months, up from 23% in 2008 (Table D2.17.1, Table D2.17.2).
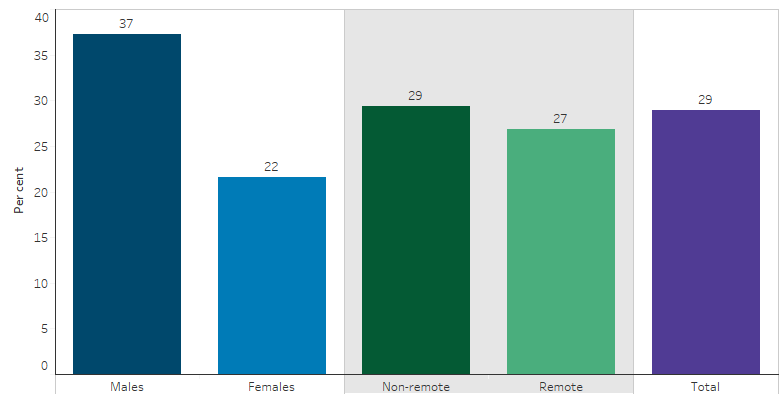
In non-remote areas (Major cities, Inner and Outer regional areas combined), 29% of Indigenous Australians aged 15 and over had used drugs or other substances in 2018−19 and in remote areas (Remote and Very remote areas combined) the proportion was 27% (Table D2.17.1, Figure 2.17.1).
Indigenous males aged 15 and over had higher rates of recent substance use than Indigenous females (37% compared with 22%) (Table D2.17.4, Figure 2.17.1).
Figure 2.17.1: Proportion of Indigenous Australians aged 15 and over who reported having used substances in the previous 12 months, by sex or remoteness, 2018–19
Source: Tables D2.17.1 and D2.17.4. AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Health Survey 2018–19.
Comparisons with non-Indigenous Australians are available from the 2019 National Drug Strategy Household Survey, which included a small sample of Indigenous Australians. Of survey participants, Indigenous Australians aged 14 and over were 1.4 times as likely to report using illicit drugs in the last 12 months compared with non‑Indigenous Australians (23% compared with 16%, respectively) (AIHW 2020).
In the 2018–19 National Aboriginal and Torres Strait Islander Health Survey, Indigenous Australians aged 25–34 had the highest rate of self- reported substance use in the last 12 months (37%) whilst those aged 55 and above had the lowest rate (15%). Indigenous males in these age brackets were 2.2 and 1.8 times more likely than Indigenous females to have used substances in the last 12 months (51% compared with 23% and 20% compared with 12%, respectively) (Table D2.17.3).
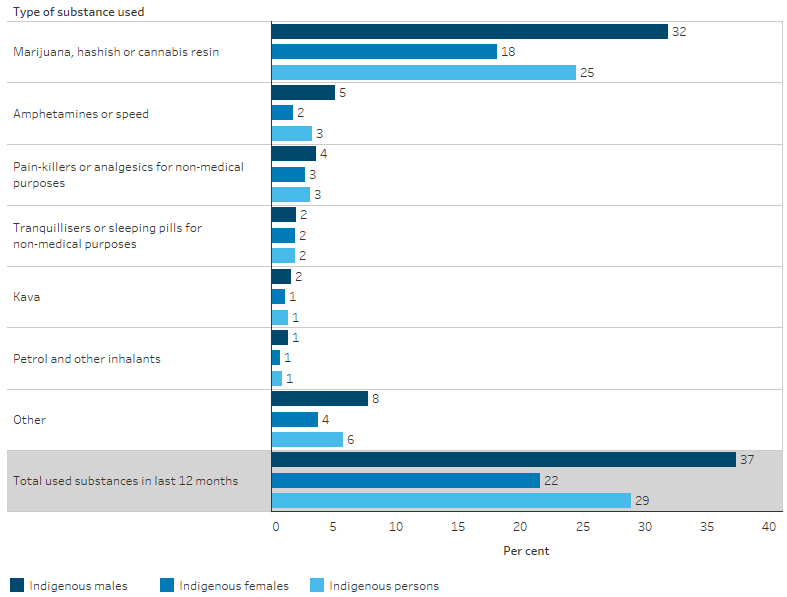
In 2018−19, marijuana, hashish and cannabis resin were the most common illicit substance used in the last 12 months for Indigenous Australians aged 15 and over (used by 25%; around 104,600 people), followed by amphetamines or speed (3%; 14,265), painkillers or analgesics for non-medical purposes (3%; 13,400) and tranquilisers or sleeping pills for non-medical purposes (2%; 8,020) (Table D2.17.1, Table D2.17.2, Figure 2.17.2). Of Indigenous Australians, 21% (87,489) reported having used only one substance in the last two months and 8% (36,003) used two or more substances (Table D2.17.5).
Figure 2.17.2: Substance used in the last 12 months, by type of substance and sex, Indigenous Australians aged 15 and over, 2018–19
Source: Table D2.17.4. AIHW analysis of the National Aboriginal and Torres Strait Islander Health Survey 2018–19.
In 2014–15, 17% of Indigenous Australians aged 15 and over reported drug-related problems as a cause of stress for themselves, family or friends in the last 12 months. Rates were similar for males (15%) and females (18%) and in remote (17%) and non-remote areas (16%) (Table D2.17.15, Table D2.17.16). Indigenous Australians reported alcohol or drug-related problems as a personal stressor at 1.3 times the rate of non-Indigenous Australians (Table D1.18.32).
In 2018–19, for Indigenous Australians aged 15 and over, those who used substances were more likely than those who did not use substances to be a current smoker (62% compared with 36%, respectively) and to drink at levels exceeding the single occasion risk (72% compared with 49%, respectively) (Table D2.17.19). In 2018−19, 2.8% of mothers with an Indigenous child aged 0−3 reported having used substances during pregnancy (Table D2.17.13).
Hospitalisations related to drug-use
From July 2017 to June 2019, there were 12,437 hospitalisations of Indigenous Australians related to drug use, accounting for 1.1% of all hospitalisations of Indigenous Australians and corresponding to a rate of 7.5 per 1,000 population. Of these hospitalisations, 59% were for mental and behavioural disorders caused by the use of substances (or 7,370 hospitalisations), 39% were due to poisoning by substances (4,828 hospitalisations), and 2% due to other direct harm (Table D1.02.1, Table D2.17.6).
Looking at the specific drugs of concern, methamphetamines was the most common drug type involved in of drug-related hospitalisations among Indigenous Australians, accounting for a quarter of these hospitalisations (25% or 3,126 hospitalisations). This was followed by cannabinoids (15% or 1,798), antidepressants and antipsychotics (12% or 1,427) and opioids (11% or 1,389) (Table D2.17.20).
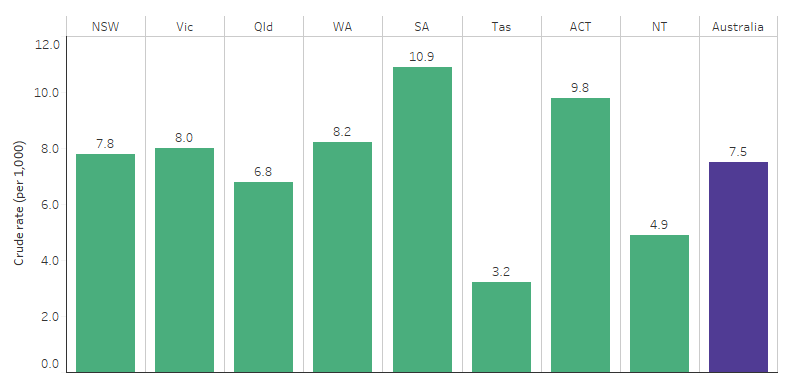
Between July 2017 and June 2019, for Indigenous Australians, the rate of hospitalisations related to drug use was 3.4 times as high for those living in South Australia compared with those living in Tasmania (10.9 and 3.2 hospitalisations per 1,000 population, respectively) These jurisdictions reflect the highest and lowest rates across all states and territories (Table D2.17.8, Figure 2.17.3). Across the states and territories, the rate of hospitalisations related to drug use was generally lower for those in remote areas than for those in non-remote areas (Table D2.17.8).
Figure 2.17.3: Hospitalisation rates for a principal diagnosis related to drug use among Indigenous Australians, by jurisdiction, July 2017 to June 2019
Source: Table D2.17.8. AIHW analysis of National Hospital Morbidity Database.
Drug use among police detainees
The Drug Use Monitoring in Australia program run by the Australian Institute of Criminology reports on drug use among police detainees at five metropolitan police stations. Of the five police stations, two were in Sydney, one was in Brisbane, one in Adelaide and one in Perth.
In 2017, the proportion of detainees who tested positive for drugs was higher for Indigenous detainees than for non‑Indigenous detainees in all five police stations (Table D2.17.12). Overall, 84% of the Indigenous detainees tested positive to a drug, compared with 73% of the non‑Indigenous detainees tested. In addition, 54% of Indigenous detainees tested positive to multiple drugs, compared with 38% for non-Indigenous detainees (Table D2.17.18).
In 2017, among detainees who provided urine at selected police stations, the two most common drugs detected for Indigenous detainees were cannabis (ranging from 52% in Sydney to 72% in Perth) and methamphetamine (ranging from 28% in Adelaide to 65% in Perth) (Table D2.17.10).
Changes over time in reported drug use and hospitalisations
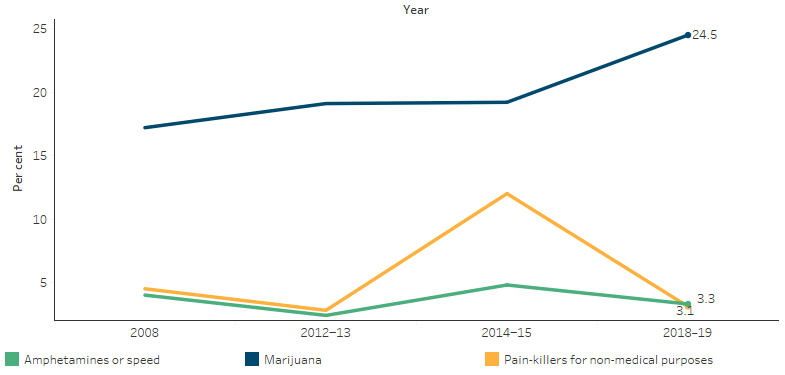
Based on data from the 2008 National Aboriginal and Torres Strait Islander Social Survey and the 2018–19 National Aboriginal and Torres Strait Islander Health Survey, there was an increase in the proportion of Indigenous Australians aged 15 and over who reported using marijuana, hashish or cannabis resin in the last 12 months. From 2008 to 2018−19, the proportion increased from 14% to 25% in remote areas and from 18% to 24% in non-remote areas.
There was a rise in the use of painkillers or analgesics for non-medical purposes by Indigenous Australians between 2008 and 2014–15 (from 5% to 12%), but the proportion was down to 3% in 2018–19 (Table D2.17.1, Figure 2.17.4). This aligns with restrictions to codeine being made a prescription-only medication from 1 February 2018 (TGA 2018).
Figure 2.17.4: Proportion of Indigenous Australians aged 15 and over who reported using a substance in the previous year, by type of substance, 2008, 2012–13, 2014–15 and 2018–19
Source: Table D2.17.1. AIHW and ABS analysis of National Aboriginal and Torres Strait Islander Social Survey 2008 and 2014–15, Australian Aboriginal and Torres Strait Islander Health Survey 2012–13 and National Aboriginal and Torres Strait Islander Health Survey 2018–19.
Looking at drug-related hospitalisations among Indigenous Australians between 2006–07 and 2018–19, the age-standardised rate increased from 3.4 to 8.1 hospitalisations per 1,000 population (linear regression analysis suggest three-fold or 214% increase) for Indigenous Australians, compared with an increase from 1.9 to 2.4 per 1,000 population (less than one-fold or 38% increase) for non-Indigenous Australians. These data relate to the six jurisdictions where the quality of Indigenous identification in the hospitals data is considered of adequate quality for all years in the time trend (New South Wales, Victoria, Queensland, Western Australia, South Australia and the Northern Territory).
Over the decade to 2018–19, the age-standardised rate of drug-related hospitalisations for Indigenous Australians increased by nearly 2.5 fold (144%, based on linear regression), compared with under one-fold (29%) for non-Indigenous Australians. As a result, the absolute difference in hospitalisation rates between Indigenous and non-Indigenous Australians increased from 1.6 to 5.7 hospitalisations per 1,000 population between 2009–10 and 2018–19 (Table D2.17.17, Figure 2.17.5). The relative difference in rates between Indigenous and non-Indigenous Australians (rate ratio) also increased over the period – from 1.8 times as high for Indigenous as non-Indigenous Australians in 2009–10, to 3.4 times as high in 2018–19 (Table 2.17.17, Figure 2.17.5).
Figure 2.17.5: Age-standardised hospitalisation rates and changes in the gap for a principal diagnosis related to drug use, by Indigenous status, NSW, Vic, Qld, WA, SA and NT, 2006–07 to 2018–19
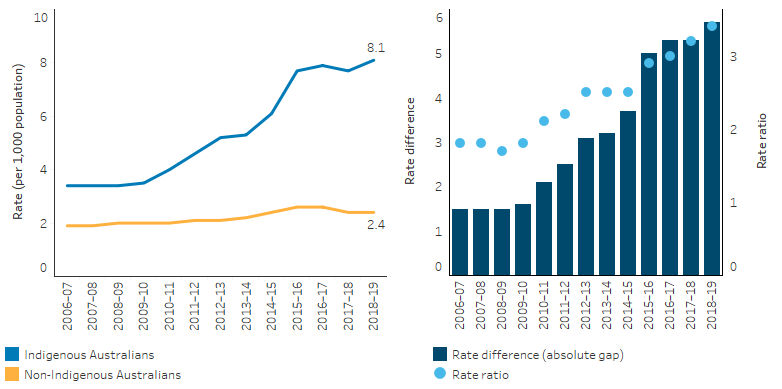
Note: Rate difference is the age-standardised rate (per 1,000) for Indigenous Australians minus the age-standardised rate (per 1,000) for non-Indigenous Australians. Rate ratio is the age-standardised rate for Indigenous Australians divided by the age-standardised rate for non-Indigenous Australians.
Source: Table D2.17.17. AIHW analysis of National Hospital Morbidity Database.
Research and evaluation findings
Harmful use of illicit drugs is more prevalent amongst Indigenous Australians than non-Indigenous Australians. Poly-drug use is also more common among Indigenous Australians and includes alcohol and tobacco, but also cannabis and other substances. In certain areas, substances such as kava and petrol sniffing are also used by Indigenous Australians (Wilkes et al. 2014).
Volatile substance use is an issue across urban, regional and remote areas of Australia and is not limited to Indigenous Australians. To address petrol sniffing as one subset of volatile substance use in regional and remote parts of Australia, since 2005, the Australian Government has supported the rollout of Low Aromatic Fuel (LAF) in place of regular unleaded petrol. Several studies show the subsidised introduction of LAF has been highly effective in reducing rates of petrol sniffing.
d’Abbs et al. (2017) examined the impact of LAF in remote Australia. LAF is used in place of regular unleaded petrol in motor vehicles and other small engines with the aim of reducing petrol sniffing in regional and remote communities across parts of the Northern Territory, Queensland, South Australia and Western Australia (d’Abbs et al. 2017). The study showed broad success in reducing petrol sniffing across the 41 Indigenous communities surveyed. Estimated petrol sniffing prevalence rates showed that between 2011–12 and 2013–14 the total number of people sniffing petrol declined by around one-third and the median petrol sniffing prevalence rate was lower in communities with LAF than in communities without LAF. For communities with data available over a longer period, the median rate of petrol sniffing fell by 96%. The study also suggested that while the fall in petrol sniffing may have been offset by increased use of cannabis and other drugs, the increase use of cannabis began before the introduction of LAF (d’Abbs et al. 2017).
Further longitudinal research in this series conducted in 2017–2018 examined the continuing impact of LAF as a deterrent to petrol sniffing in Australian communities. Findings were based on fieldwork conducted in 25 communities. Comparable data from four previous surveys is available in 11 of the 25 communities included in the study. In these 11 communities, from 2006 to 2018 the total estimated numbers of people currently sniffing petrol dropped from 453 to 22, a decline of 95.2%. In 22 of the 25 communities, comparison can be made between petrol sniffing prevalence in 2013–14 and 2017–18. Across the period, total numbers in these 22 communities fell from 227 to 109, a decrease of 52% (d'Abbs & Shaw 2016; University of Queensland 2019).
The study demonstrates the long-term benefits of continuing to make LAF available and suggests that if LAF was removed from communities, there would be a significant risk of petrol sniffing returning. The availability and use of youth engagement activities, such as sport and recreation in communities was also shown to be an important influence on reducing the demand for petrol and other volatile substances as well as other drugs among young people (University of Queensland 2019).
Methamphetamine use in Australia has been increasing, and there has been a shift towards using the more dangerous form, crystalline methamphetamine (ice). A Review of methamphetamine use among Indigenous Australians, found that the use of, and harms associated with methamphetamine are more prevalent among Indigenous Australians than non-Indigenous Australians, with historical factors such as colonisation and disempowerment; and social factors, such as housing, education and employment, being major influences. Major harms associated with methamphetamine use include an increased risk of stroke (and other cardiovascular problems), dependence, psychosis, aggression, violence, overdose and death (Snijder & Kershaw 2019).
A cross-sectional survey of Indigenous youth aged 16–29 in 2011–13 found that just over 35% had used an illicit substance in the last year. Cannabis was the most frequently used, with around 30% of respondents having used this drug in the previous 12 months. Weekly or more frequent use of cannabis was reported by 18% of participants in urban areas, 22% in regional and 14% in remote areas (the remote sample was small and results should be interpreted with caution). Around 11% reported using ecstasy in the last year, followed by amphetamines (9%) and cocaine (4%). The injection of drugs was reported by 3% of respondents, most commonly methamphetamine (37%), heroin (36%) and methadone (26%) (Ward et al. 2014).
Indigenous Australians’ greater exposure to life stressors, traumatic events and associated drug and alcohol use are all factors associated with social and emotional wellbeing (Dudgeon et al. 2017). Self-harm, homelessness and incarceration can both precede and be a result of drug and alcohol use (Nathan et al. 2020). Several studies have linked marijuana use to increased risk for psychiatric disorders including psychosis, depression and anxiety, with the link being more prominent in those with a pre-existing genetic or other vulnerability (NIDA 2020; Radhakrishnan et al. 2014). Harmful levels of alcohol and drug use by Indigenous Australians have also been noted in the majority of Indigenous suicide clusters (Dudgeon et al. 2017).
Geia et al. (2018) conducted a systematic review of literature evaluating the impact of substance use programs on Australian Indigenous youth. The study focuses on demand control programs and the authors note the better outcomes from interventions that are culturally safe, closely involved with local communities and delivered by Indigenous community-controlled organisations with support to develop the capacity and own the intervention (Geia et al. 2018).
Project Ice Mildura is a community-based campaign established in 2013 with an aim to raise awareness in the community about the harmful effects of ice (crystalline methamphetamine). An evaluation of the program showed that it was successful in raising awareness and understanding within the community about ice, and in taking action regarding issues relating to the drug. As a result of its success, the program was extended. Recommendations from the evaluation included initiating discussions with relevant government bodies on the lack of appropriate withdrawal and rehabilitation services specific to ice users. Suggestions were also put forward for other communities wanting to replicate similar projects. These include developing and implementing evaluative tools alongside the planning and creation of community approaches for raising awareness and understanding (Harley et al. 2014).
Nagel et al. (2009) developed and evaluated a culturally adapted mixed-methods intervention to address chronic mental illness and comorbid substance use among Indigenous Australian patients (Nagel et al. 2009). The intervention consisted of treatment sessions and explored family support, strengths, stresses and goal setting. Evaluation of the intervention showed that the intervention group had improved mental health and substance use outcomes compared with the treatment as usual group. The improvement was also sustained over time, suggesting that brief interventions that address co-morbid disorders in an integrated way can result in significant change (Nagel et al. 2009).
In 2017, the Department of the Prime Minister and Cabinet commissioned the National Drug and Alcohol Research Centre (NDARC) to undertake a community based participatory research project of Indigenous Alcohol and Other Drugs Residential Rehabilitation (IAODRR) services in New South Wales. The purpose of the research project was to standardise data collection processes and models of care to inform the evidence base for Indigenous AOD residential rehabilitation services in New South Wales.
The project identified the need to standardise data collection by embedding evaluation capacity into IAODRR services. Key outcomes of the project were:
- a standardised assessment tool for collecting client data on substance use, mental and physical health, quality of life and cultural connectedness;
- a program logic model to define core treatment and organisational components for IAODRR services;
- a standardised approach for follow-up support including client exit interview and assessment, referral, follow up contact and assessment; and
- the development of an evaluation framework to evaluate costs and benefits of IAODRR services (Shakeshaft 2018).
Implications
Harmful drug and other substance use has a significant impact on people’s lives and commonly occurs with other conditions, including mental health disorders and suicide. It is therefore crucial that treatment and rehabilitation services complement broader initiatives, particularly given the increasing use of drugs such as marijuana among Indigenous Australians and the risk this can pose for people vulnerable to psychiatric disorders (NIDA 2020; Wilkes et al. 2014). Supply reduction strategies have also been found to be successful, for example in the case of replacement of regular unleaded petrol with low aromatic fuel to reduce petrol sniffing, and should be considered where possible (Wilkes et al. 2014).
For Indigenous Australians, substance use may be exacerbated by increased vulnerability that has resulted from the legacies of colonisation, inequality and racism. These issues make it vitally important for the provision of culturally safe and trauma informed treatment and healing services (Atkinson 2013). Services also need to recognise culture as a central component, and reinforce Indigenous family systems of care and support, and promote community ownership and control (Wilkes et al. 2014).
Strategies should address underlying social determinants (including inadequate housing, education, employment and income), aim to prevent the uptake of harmful substance use, provide treatment for those who are dependent, and support those whose lives are affected by others’ harmful AOD use (Gray et al. 2018).
References
-
ABS (Australian Bureau of Statistics) 2016. National Aboriginal and Torres Strait Islander Social Survey, 2014–15. Canberra: ABS.
-
AIHW (Australian Institute of Health and Welfare) 2018. Impact of alcohol and illicit drug use on the burden of disease and injury in Australia: Australian Burden of Disease Study 2011. Canberra: AIHW.
-
AIHW 2020. National Drug Strategy Household Survey 2019. Drug Statistics series no. 32. PHE 270. Canberra.
-
AIHW 2022. Australian Burden of Disease Study: Impact and causes of illness and death in Aboriginal and Torres Strait Islander people 2018. Canberra: AIHW.
-
Atkinson J 2013. Trauma-informed services and trauma-specific care for Indigenous Australian children. Closing the Gap Clearinghouse. Canberra: Australian Institute of Health and Welfare & Australian Institute of Family Studies.
-
Catto M & Thomson N 2008. Review of illicit drug use among Indigenous peoples. Australian Indigenous HealthInfoNet.
-
d'Abbs P & Shaw G 2016. Monitoring trends in the prevalence of petrol sniffing in selected Australian Aboriginal communities 2011-2014: Final Report. Darwin: Menzies SHR.
-
d’Abbs P, Shaw G & Field E 2017. The impact of subsidized low aromatic fuel (LAF) on petrol (gasoline) sniffing in remote Australian indigenous communities. Substance Abuse Treatment, Prevention, and Policy 12:38.
-
Dudgeon P, Calma T & Holland C 2017. The context and causes of the suicide of Indigenous people in Australia. Journal of Indigenous Wellbeing 2:5-15.
-
Geia L, Broadfield K, Grainger D, Day A & Watkin‐Lui F 2018. Adolescent and young adult substance use in Australian Indigenous communities: a systematic review of demand control program outcomes. Australian and New Zealand journal of public health 42:254-61.
-
Gray D, Cartwright K, Stearne A, Saggers S, Wilkes E & Wilson M 2018. Review of the harmful use of alcohol among Aboriginal and Torres Strait Islander people. Australian Indigenous HealthInfoNet.
-
Harley F, Forbes C & Cordoma L 2014. Project Ice Mildura Evaluation of the community campaign measuring reach and impact. Mildura, Victoria: Vinson Centre for Applied Social Research and Mallee Family Care.
-
Karam J, Sinclair G & Rackstraw L 2014. Dignity, Diversion, Home and Hope: A Review of Interventions for Volatile Substance Misuse in Regional North Queensland. (ed., Department of the Prime Minister and Cabinet). Canberra: DPMC.
-
Kratzmann M, Mitchell E, Ware J, Banach L, Ward J & Ryan J 2011. Injecting drug use and associated harms among Aboriginal Australians. Canberra: ANCD.
-
Midford R, MacLean S, Catto M, Thomson N & Debuyst O 2011. Review of volatile substance use among Indigenous people. Australian Indigenous HealthBulletin 11.
-
Nagel T, Robinson G, Condon J & Trauer T 2009. Approach to treatment of mental illness and substance dependence in remote Indigenous communities: results of a mixed methods study. Australian Journal of Rural Health 17:174-82.
-
Nathan S, Maru K, Williams M, Palmer K & Rawstorne P 2020. Koori voices: self-harm, suicide attempts, arrests and substance use among Aboriginal and Torres Strait Islander adolescents following residential treatment. Health & Justice 8:4.
-
NIDA 2020. Marijuana Research Report: Is there a link between marijuana use and psychiatric disorders? .
-
Radhakrishnan R, Wilkinson ST & D’Souza DC 2014. Gone to pot–a review of the association between cannabis and psychosis. Frontiers in Psychiatry 5:54.
-
Robinson G, Silburn S & Leckning B 2011. Suicide of Children and Youth in the NT 2006-2010: Public Release Report for the Child Deaths Review and Prevention Committee. Darwin: Menzies SHR.
-
SCRGSP 2014. Report on Government Services 2014. Canberra: Productivity Commission.
-
Shakeshaft A, Clifford A, James D, Doran C, Munro A, Patrao T, Bennett A, Binge C, Bloxsome T, Coyte J, Edwards D, Henderson N, Jeffries D. 2018. Understanding clients, treatment models, and evaluation options for the NSW Aboriginal Residential Healing Drug and Alcohol Network (NARHDAN): a community-based participatory research approach. National Drug and Alcohol Research Centre (UNSW Sydney).
-
Snijder M & Kershaw S 2019. Review of methamphetamine use among Aboriginal and Torres Strait Islander people. Australian Indigenous HealthInfoNet.
-
TGA (Therapeutic Goods Administration) 2018. Codeine information hub: changes to patient access for medicines containing codeine. Canberra: Australian Government Department of Health and Aged Care.
-
University of Queensland 2019. Longitudinal research into petrol sniffing and other substance abuse trends in Indigenous communities: final report. Queensland.
-
Wand H, Ward J, Bryant J, Delaney-Thiele D, Worth H, Pitts M et al. 2016. Individual and population level impacts of illicit drug use, sexual risk behaviours on sexually transmitted infections among young Aboriginal and Torres Strait Islander people: results from the GOANNA survey. BMC Public Health 16:600.
-
Ward J, Bryant J, Wand H, Pitts M, Smith A, Delaney-Thiele D et al. 2014. Sexual health and relationships in young Aboriginal and Torres Strait Islander people: results of the first Australian study of knowledge, risk practices and health service access for sexually transmissible infections (STIs) and blood borne viruses (BBVs) among young Aboriginal and Torres Strait Islander people: The Goanna Survey. Alice Springs: Baker IDI Heart & Diabetes Institute.
-
Wilkes E, Gray D, Casey W, Stearne A & Dadd L 2014. Harmful substance use and mental health. Working together: Aboriginal and Torres Strait Islander mental health and wellbeing principles and practice. 2nd edition ed. Canberra: Department of The Prime Minister and Cabinet:125-46.