
Acute rheumatic fever and rheumatic heart disease
Rheumatic Heart Disease (RHD) is a disease of disadvantage that is both preventable and treatable. RHD is caused by damage to the valves of the heart as a result of one or repeated episodes of acute rheumatic fever (ARF). Both ARF and RHD are associated with socioeconomic and environmental factors such as poverty and overcrowded housing (AIHW 2023b; Coffey et al. 2018).
Over the 5-year period from 2017 to 2021, in the 5 jurisdictions with state-based ARF and RHD registers (New South Wales, Queensland, Western Australia, South Australia, and Northern Territory), 2,570 cases of ARF were diagnosed among First Nations people (69 cases per 100,000 population). First Nations people accounted for 92% of all ARF cases (2,570 of 2,781 cases, excluding cases where Indigenous status was unknown).
Of 2,570 ARF cases among First Nations people:
- 71% (1,814 cases) were first known episodes
- 28% (728 cases) were recurrent (a repeated episode of ARF or had existing RHD)
- 44% (1,142 cases or 140 per 100,000) occurred among First Nations children aged 5–14, the highest of any age group.
As at 31 December 2021, in the 4 jurisdictions where ARF and RHD register data were available for people of all ages (Queensland, Western Australia, South Australia, and Northern Territory), nearly 8 in 10 (78%, 5,221) people with RHD were First Nations people (1,080 cases per 100,000 population).
The proportion of all RHD cases among First Nations people was highest for those aged 35 and over (45% or 2,366) followed by those aged 15–34 (44% or 2,305). In the 3 jurisdictions where data are available by sex (Queensland, South Australia, and Northern Territory), the rate of RHD was around twice as high for First Nations females as for First Nations males.
Antibiotics (Benzathine Penicillin G or BPG) can be given to people who have been diagnosed with ARF and/or RHD to prevent further Strep A infections, thereby reducing the risks of developing ARF again and of developing or worsening RHD. In 2021, in Queensland, Western Australia, South Australia and the Northern Territory combined, of the 4,816 First Nations people who were prescribed antibiotics as secondary prophylaxis, 31% (1,513) received at least 80% of the prescribed doses.
Between July 2017 and June 2019, 1,428 First Nations people were hospitalised for ARF or RHD, a rate of 86 per 100,000 population. Among the 5 jurisdictions (New South Wales, Queensland, Western Australia, South Australia, and Northern Territory), the Northern Territory (481 per 100,000) had the highest rate, followed by Western Australia (108 per 100,000). Hospitalisation rates for ARF or RHD were higher for First Nations people living in remote areas (Remote and very remote areas combined) than for those living in non-remote areas (Major cities, inner regional and outer regional areas combined) (330 per 100,000 compared with 30 per 100,000) (Figure 4.20).
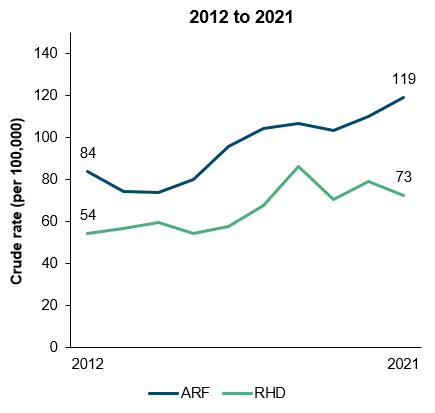
Over the decade from 2012 to 2021, in the 4 jurisdictions with data available (Queensland, Western Australia, South Australia, and the Northern Territory combined), the incidence rates of ARF and RHD among First Nations people both increased. The incidence rates of ARF among First Nations people increased from 84 per 100,000 to 119 per 100,000 population, driven by an increase in the Northern Territory, where the rate of ARF approximately doubled (108% increase, based on linear regression analysis). The incidence rates of RHD among First Nations people fluctuated between 54 and 86 new cases per 100,000 population with an overall upwards trend. Based on linear regression, there was a 50% increase in the rate of RHD, reflecting increases in RHD incidence in the Northern Territory (98% increase), and in Queensland (40% increase) (Figure 4.20).
Note that the increase may reflect a real increase in the number of cases occurring, but may also be due to improved detection and diagnosis of cases, increases in the number of people being recorded on the registers, or a combination of these.
Figure 4.20: Hospitalisations for ARF/RHD by remoteness (2017–2019)(a), and incidence rates of ARF and RHD over time (2012 to 2021)(b), among First Nations people
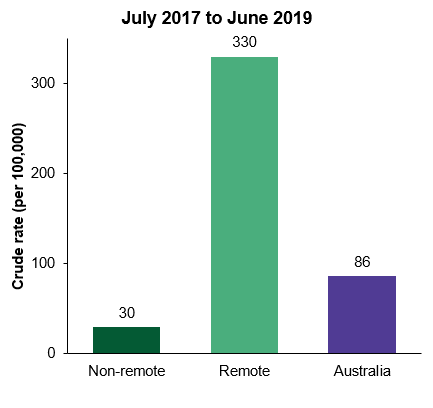
(a) Data shown for hospitalisations of ARF/RHD are from all jurisdictions combined.
(b) Data shown for incidence rates of ARF and RHD are from Queensland, Western Australia, South Australia, and the Northern Territory combined.
Source: Measure 1.06, Table D1.06.6, Table D.06.15, Table D1.06.17 – National Hospital Morbidity Database & National Rheumatic Heart Disease data collection.
For further information, see: