
Birthweight
Being born with a healthy birthweight provides children with the best start in life, while low birthweight infants are prone to ill-health in childhood and to chronic disease as adults (AIHW 2011). The importance of healthy birthweight is also reflected in Target 2 of the National Agreement: By 2031, increase the proportion of Aboriginal and Torres Strait Islander babies with a healthy birthweight to 91 per cent – see the Closing the Gap Information Repository.
In this report, birthweight is categorised as follows:
- low birthweight: less than 2,500 grams
- healthy birthweight: 2,500 to 4,499 grams
- high birthweight: 4,500 grams or more.
Most First Nations babies are born with a healthy birthweight, but the rate of low birthweight among First Nations babies remains about twice as high as for non-Indigenous babies.
In 2020, almost 9 in 10 (88.9%) singleton First Nations babies were born with a healthy birthweight, while 9.6% had a low birthweight, and 1.4% had a high birthweight. In comparison, 94.0% of non-Indigenous babies had a healthy birthweight, 4.7% had a low birthweight, and 1.2% had a high birthweight.
The average birthweight of singleton First Nations babies in 2020 was 3,271 grams, compared with 3,367 grams for non-Indigenous babies.
Over the period 2013 to 2020, the proportion of First Nations babies born with a healthy birthweight did not change significantly, ranging between 88.7% and 89.5%.
In 2020, the national rate of low birthweight for First Nations babies was 9.6%, ranging from 8.4% in South Australia to 14.6% in the Northern Territory. The rate of low birthweight babies born to First Nations mothers also varied with remoteness areas. Comparing with First Nations babies in the Major cities (8.3%), rates were higher for those living in the Outer regional (9.5%), Remote (13.2%) and Very remote (13.1%) areas. There was no significant difference in rates between Major cities and Inner regional areas (8.3% and 9.1%, respectively) (Figure 4.3).
Figure 4.3: Low birthweight by Indigenous status of baby (2013–2020), and low birthweight by remoteness for First Nations babies (2020)
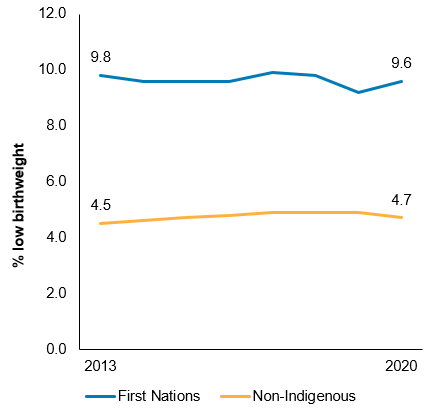
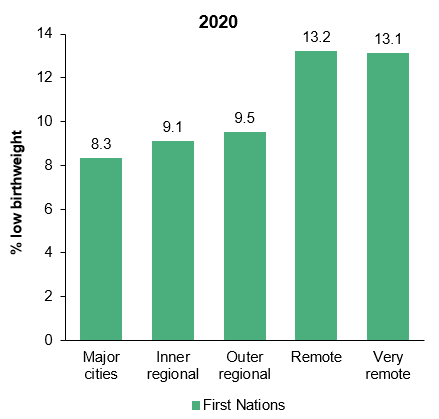
Source: Measure 1.01, Table D1.01.20 and Table D1.01.22 – AIHW analysis of the National Perinatal Data Collection.
Antenatal care includes risk identification, prevention and management of pregnancy-related or concurrent diseases, health education and health promotion. Regular antenatal care that commences early in pregnancy has been found to have a positive effect on health outcomes for mothers and babies (AHMAC 2012).
Among First Nations mothers who gave birth at 20 weeks or more gestation in 2020, 71% received their first antenatal care visit in the first trimester (14 weeks). In 2020, 88% of First Nations mothers who gave birth at 32 weeks or more attended 5 or more antenatal visits throughout their pregnancy. Between 2012 and 2020, based on age-standardised rates, the proportion of mothers who attended first antenatal care in the first trimester of their pregnancy increased by 41% for First Nations mothers and by 33% for non-Indigenous mothers (Figure 4.4).
First Nations mothers who attended their first antenatal care visit in the first trimester of pregnancy were less likely to have a low birthweight baby compared with those who either had their first visit after 20 weeks of pregnancy or did not have any antenatal care (9.2% compared with 14%) (Figure 4.4).
Figure 4.4: Antenatal care visit during the first trimester by Indigenous status (2012 to 2020) (age-standardised), and low birthweight First Nations babies by duration of pregnancy at first antenatal visit (2020)
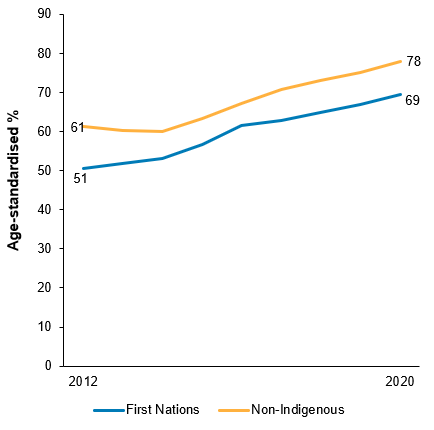
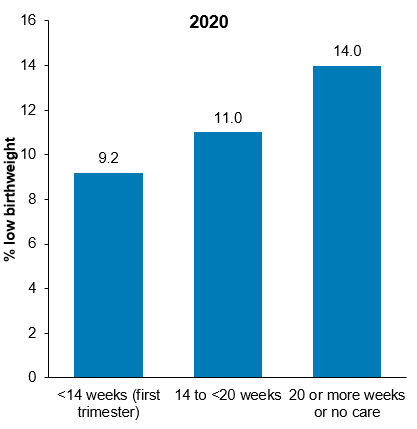
Note: Data on the duration of pregnancy at first antenatal care visit and birthweight status of babies refer to mothers who gave birth at 20 weeks or more gestation.
Source: Measure 3.01, Table D3.01.21 and Table D3.01.14 – AIHW analysis of the National Perinatal Data Collection.
During pregnancy, smoking is associated with an increased risk of low birthweight in babies (see Key factors contributing to low birthweight of Aboriginal and Torres Strait Islander babies). In 2020, the proportion of low birthweight babies born to First Nations mothers who smoked was 2.6 times as high as for those born to First Nations mothers who did not smoke (14.3% and 5.5%, respectively). Over the period from 2011 to 2020, the age-standardised proportion of First Nations mothers who smoked during pregnancy decreased by 4 percentage points (from 48% to 44%).
For further information, see: